“Bessel van der Kolk wants to change the way we heal a traumatized mind — by starting with the body,” reports Jeneen Interlandi in the New York Times Magazine May 22. (Dr. van der Kolk in session drawn by Matthew Woodson for the Times.)
“Trauma has nothing whatsoever to do with cognition,” van der Kolk says. “It has to do with your body being reset to interpret the world as a dangerous place.” That reset begins in the deep recesses of the brain with its most primitive structures (brain stem), regions that, he says, no cognitive therapy (frontal cortex) can access.
“It’s not something you can talk yourself out of.”
OK, it’s a bit off my topic. The Times doesn’t mention attachment trauma, although van der Kolk talks about that constantly. As to healing, it focuses on adult war PTSD. It only speaks to child trauma by debating what a child abuse victim can and can’t remember (not much of a call to heal child trauma).
But Ms. Interlandi does let van der Kolk speak to his charge that there is a lot more trauma than we think, and that standard “cognitive” treatments are not working. “Patients are still suffering, and so are their families. We need to do better,” van der Kolk says.
“Van der Kolk says he would love to do large-scale studies comparing some of his preferred methods of treatment with some of the more commonly accepted approaches,” she points out. “But funding is nearly impossible to come by for anything outside the mainstream. In the wake of the Sept. 11 terrorist attacks, he says, he was invited to sit on a handful of expert panels. Money had been designated for therapeutic interventions, and the people in charge of parceling it out wanted to know which treatments to back.
To van der Kolk, it was a golden opportunity. We really don’t know what would help people most, he told the panel members. Why not open it up and fund everything, and not be prejudiced about it? Then we could study the results and really learn something. Instead, the panels recommended two forms of treatment: psychoanalysis and cognitive behavioral therapy.
“So then we sat back and waited for all the patients to show up for analysis and C.B.T. And almost nobody did.” Spencer Eth, then medical director of behavioral health services at St. Vincent’s Hospital in Manhattan, (later) gathered data on the mental-health care provided to more than 10,000 Sept. 11 survivors.
The most popular service by far was acupuncture. Yoga and massage were also in high demand. “Nobody looks at acupuncture academically,” van der Kolk says. “But here are all these people saying that it’s helped them.”
Out of 208 reader comments to the Times, I only found two that weren’t deeply grateful for his approach, as I am. These two didn’t mention healing either.
Enjoy reading about Dr. van der Kolk today, but read carefully – the Times, ever a bit arrogant, puts in some gnarly innuendos I didn’t like, which the two comments made worse. So I had to do further research on this one. My results to come next week…
—————————–
Kathy’s news blogs expand on her book “DON’T TRY THIS ALONE: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
“Why Empathy is Essential – and Endangered”
Address to The National Council for Behavioral Health
Washington, DC, May 4, 2014 – Click link or photo for video https://www.youtube.com/watch?v=M6kDeBaJi0M
“Empathy is what makes us human,” says brain scientist Dr. Bruce Perry, MD – but this has not sunk in for Americans. If simple kindness isn’t enough, what about the minor fact that it’s brain science? Or that by ignoring this basic fact, we’re violating biology, so we’re dying as a species?
To let Dr. Perry make his point, today I’ve just got a few quotes from his May 4 Washington DC address, to provoke you to watch the video kindly posted by the National Council for Behavioral Health.
”From birth, we seek intimate connections, bonds made possible by empathy — the ability to love and to share the feelings of others,” Perry begins. But “our policies routinely violate the biological reality of empathy, and that’s destructive…
“For example, we pass on to the next generation explicit choices that we’re going to teach math — but not music…We don’t care if everyone learns to read and perform music or not, but they’ve got to do arithmetic… We have extensive rules for all the things everyone has to learn to drive a car… but we don’t do the same for raising a child! We don’t make any systematic recommendations, or ensure that everybody who’s about to have a child has the fundamental knowledge of what’s necessary for the child…
“We’re exposing our children to levels of violence as a problem solving technique, at rates that are at least 50 times greater than alternate methods of problem-solving…
“We have invented ourselves into a corner with technology… into models of child rearing, education, and building communities that is fundamentally disrespectful of two of the greatest (biological) gifts our species has: the fundamental malleability of the human brain in early life, and the fundamental relational (empathic) nature of human beings…. As a result we are much more vulnerable to mental health, social health, cognitive health, and physical health problems.
Humans Need Humans Around to Live
“Human beings are biological creatures with genetic gifts… The only way we survived was by forming relationships, collaborative relationships… Human beings are neurobiologically meant to be connected to others: to live, work, hunt, play, invent, and die in groups.
“We use the word ‘independent’ a lot — but the truth is there’s not a single human on this planet, ever, that’s been independent. All of our physiology is designed to connect to others, we have huge parts of our brain designed purely to respond to the non-verbal cues of others… it’s in the way our face is oriented, our facial configuration is forward, looking at people… We have sensory apparatus on our skin that’s meant to be touched… so that we can feel somebody caress us…
“Our brain is a social organ; we are social animals. We don’t have any natural body armor, camouflage, stinging other things. We form groups! Human beings are ‘meat on feet’ to the natural world! The only way we survive is by forming collaborative groups, by sharing what we hunted and what we gathered with everybody else in our group. And the typical living group was a developmentally heterogeneous, multi-family, multi-generational group: 40 to 50 people.
“And in that group… the ratio of developmentally more mature individuals who cared for you, protected you, nurtured you… was four to one. But now, we think it’s an incredibly enriched early child care environment if there’s one caregiver to six kids! That’s 1/24 the relational density the brain benefits from…
“Today, the whole organization of society flies in the face of this… In the last census, one third of American households were oneperson.
“On top of which, now… the typical American spends 11 hours a day interacting with digital devices, and not with fleshy objects! And I want to talk about the consequences of this for how we end up expressing our ability to be compassionate (or not)…. You see it all the time, complaints in the psychological literature about the disconnectedness of multi-tasking constantly with our phones… but we do it ourselves… You’re talking to someone, then your phone will vibrate — and it pulls you away from them.
” It breaks the rhythm of social contact, of empathic engagement– and the truth is: those things are physiologically meaningful.”
—————————–
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
In March 2013, I was standing unknown in a crowd of professors and therapists at a UCLA conference, and noticed a quiet gentleman on my right. I’d seen his photo online. “Dr. Schore?” I asked. “Yes,” said Allan Schore, turning calm eyes on me.
“I’m so grateful for all you’ve done to show that babies can’t control emotions, that’s the mother’s job to model, and emotions are ok,” I blurted, suddenly in tears. “I’m writing a book on what it feels like on the inside, when we don’t get that as an infant.”
Dr. Schore didn’t flinch; his eyes grew wide with empathy. He got it. He got a total stranger, right by the conference stage, got that I had walked through a hell of emotional pain to study this. He got that I was feeling love for him because he’s shown there’s a scientific reason for the pain. He got that “emotions are ok” and only emotions from a caring other can heal this, so he gave me emotions: presence and compassion. On the spot. “We see it every day,” he said.
Just sayin’: he walks the walk.
UCLA professor Allan Schore is a world leader in Attachment Theory. He’s known as “the American Bowlby” after British psychiatrist John Bowlby who first wrote about attachment in the 1950s. [FN1] Schore was among the first to put together the latest brain science on how an infant’s brain forms biologically (“developmental neuroscience”), with the early psychology of the infant mind (“developmental psychoanalysis”).
Dr. Schore’s 9-28-14 Oslo speech “The Most Important Years…the Right Brain and Its Importance” is a must-see to understand infant developmental trauma. He calls it “trauma in the first 1000 days, conception to age two.” Schore reviews how the theories he’s published since the 1990s are being proven to be hard science by today’s brain scan technologies (content starts minute 8): https://www.youtube.com/watch?v=KW-S4cyEFCc
Schore is known for documenting the “origin of the self”– what, scientifically, is the “Self”? What is it that makes me, Me?
He calls it “the origin of the early forming subjective implicit self.” It’s entirely subjective; each infant has a different experience. It’s “implicit memory” because the self forms in infancy when memory is only subconcious. It all happens years before we have thought and conscious “explicit memory” at age two or three.
This isn’t mere geek-speak; the mental, emotional, and physical health of all humans depends on it. We can’t remember what happened before age 3 when our self was formed, but the experience had massive impact. It’s all still “down there,” driving our feelings and behavior big time for the rest of our lives.
When the self is damaged during formation in early infant and childhood, a person can feel miserable all their life. The ACE Study shows this often leads to biological disease and premature death.
The Self and Emotions : Secure Attachment
Babies are born with a massive level of emotions. Schore reports that they are overwhelmingly dependent on the mother to show them how to handle it all. An infant’s brain doubles in size “from the last trimester of pregnancy through the second year,” he says. “At birth, there are hardly any cortical (conscious thinking brain) areas that are myelinated and online… so it’s impossible for the baby to regulate its own emotions…
“The mother is the regulator of that baby,” he says, and this shapes the development of its entire brain. “Over the first year… the mother’s interactions are shaping the very wiring of those higher regulatory centers… Attachment communications which are emotional are forging the connections in the early developing right brain… The right brain literally is imprinted by these attachment relationships while it is being created…” FN2
It’s all subconscious. With “secure attachment,” when a baby cries, the mother “attunes” to it. An “attuned” mother doesn’t say “think” or “ought to.” She feels a strong, emotional urge to comfort her baby; she subconsciously intuits whether her baby cries because it’s hungry, wet, or tired. “The mother is able to pick up the baby’s communications,” Schore says. “She is not doing this by language, there is no thinking or language before age two. She is picking up bodily-based nonverbal communications: facial gestures, auditory tone of voice, and tactile expressions. The attachment communication is more than between the mother and the infant’s minds; it’s between their bodies…
“She is psychobiologically attuning to the internal rhythms… of the baby’s autonomic nervous system and central system arousal… It’s an attunement of mind and body. In doing so, she is regulating the baby’s rhythms and allowing the baby to create different emotional states that are associated with these different rhythms. This is not a matching of behavior; it is more of an intuitive matching of the internal rhythms of the baby.
“The baby is expressing these internal rhythms through the emotional communications it is sending back to the mother, in the prosody of the baby’s voice, or in the cry, or in the expression on the baby’s face, or in the gesture. They are matching each other’s subjective state. Now, when two people match their subjective states, there is a sense of empathy, there is a sense of a bond; a sense that ‘someone’s body is exactly resonating with my body.’ When that occurs there is an amplification of arousal, and this amplification of arousal leads to things like joy states.”
Infants also have no sense of self. Instead, Schore adds, there’s a “mother-baby continuum” for at least the first six months of life where the “dyad” (mother and child) often don’t know (and don’t care) where one person ends and the other begins.
We begin life as a sea of emotions, and then mom models for us again and again, that she can comfort our wild emotions. Unconsciously we pick up that skill. After we cry and mom comforts us for the millionth time, one day we feel our way to stop crying because we’ve “internalized” mom’s comfort. We subconsciously learn to manage emotions, to both enjoy good emotions, and also–very important–to tolerate and be able to fully feel negative emotions. Without fearing or repressing them.
This is also called “Emotional Object Constancy.” Mom was an external object, but now we’ve taken her image inside us, so we feel loved and emotionally secure 24×7, even when we’re alone.
Our “self” begins when we first start to “regulate” our own emotions (“affect”) this way. When we realize we can feel our emotions and also modulate them, without screaming for someone else to do it for us? That’s when we first realize that we are not merely part of mom. We’ve got some independent “self.” “Essentially, one’s self-concept is focused around a positive sense of emotionality in the self,” says Schore.
Insecure Attachment and Trauma
Or not.
Back to how all babies are born with a massive level of emotions. We’re all supposed to receive all that attuning above, then we’re fine.
Or not.
What if we’re an “Or Not” baby? What if we cry but no one comes? Or what if someone comes, but they don’t have the neural equipment to attune, or they’re too distressed to attune? “That baby learns that there is no comfort, that emotions are terrifying, and the world is a scary place,” Dr. Schore says. His colleague Dr. Ed Tronick shows this graphically in the “Still Face Experiment”– click for video. [FN3]
That baby often does not develop much of a self. To the extent no one showed it how to manage emotions, the day could not come when it could “regulate like mom.” It can’t regulate, so it can’t individuate.
That is really uncomfortable; it’s what’s behind the feeling that “I have a hole in me.”
All the above leave deep damage, even just passively.
Plus, on top of that: what if we cry, someone comes, and then there’s active aggression; we’re yelled at or physically maltreated?
A whole lot can and does go wrong for a baby. I call that a lot of Adverse Infant Experiences (AIE). “Aaiiee!” Double ouch.
Schore says this is the root of developmental trauma. “In trauma there is an intense negative state about the sense of self,” he says, with “extremely high states and low states of arousal, an inability to internally regulate their state or to use other people to help them regulate their state and bring them into a sense of comfort.”
With insecure attachment, he says, “there are problems that the caregiver is having emotionally… There is anxious insecure attachment, where the mother is preoccupied or unpredictable… There is also avoidant insecure attachment, where the mother is mostly cold…
“And there is ‘mind blindness,’ so to speak. There are some mothers who cannot read the tone of the baby… depressive mothers have problems reading facial expressions, especially the facial expressions and gestures of the baby. You see inter-generational transmission of these deficits…”
Schore first showed this scientifically in his three blockbuster books Affect Regulation and the Origin of the Self (1994), Affect Dysregulation and Disorders of the Self, and Affect Regulation and the Repair of the Self. FN4
“Affect regulation” means we can freely feel our emotions without being emotionally blocked, we can enjoy our emotions–yet also be “on top”of our emotions, so they don’t feel overwhelming, painful or frightening. If not, we suffer “affect dysregulation ” i.e., some level of painful emotional chaos.
We all know people who either can’t or won’t access their emotions, or others whose emotions go out of control to where they and those around them feel miserable. Others swing to both extremes, but never simply enjoy their emotions without freaking out or hurting people.
The good news is: there is repair, as Dr. Schore’s third book lays out in detail. At a support group, Al Anon meeting, therapist’s office, or with friends, repair means we find other humans to do exactly what Schore did for me on the floor of that conference: be present emotionally with another emotionally-attuned human being.
If we can sit for an hour and attune to another human willing to share our emotion state and help us learn to gradually shift and modulate it, we learn to “regulate.” Brain scans now show that we can literally repair the neural circuits which remained painfully out of tune when we didn’t receive human attunement as kids.
It takes time, perseverance, courage, and real human beings like Allan Schore. I’ve met them–they’re out there. Find them.
——————-
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
Footnotes
FN1 Bowlby, John, “The Nature of a Child’s Tie to His Mother,” British Psychoanalytical Society, London, 1958; “Attachment and Loss,” New York, Basic Books, 1969
FN2 Schore, Allan N., PhD, “Affect Regulation and Mind- Brain-Body Healing of Trauma,” National Institute for the Clinical Application of Behavioral Medicine (NICABM), June 15, 2011
— Schore, Allan N., “The right brain implicit self lies at the core of psychoanalysis,” Psychoanalytic Dialogues 21:75–100, 2011 www.lifespanlearn.org/documents/2011Handouts/Schore/Schore%20Psych%20Dialogues%2011.pdf
—Interview with Allan Schore – ‘the American Bowlby,’ by Roz Carroll, UK ; The Psychotherapist, Autumn 2001, www.thinkbody.co.uk/papers/interview-with-allan-s.htm
FN3 Dr. Ed Tronick of the U Mass Boston’s Infant-Parent Mental Health Program did his first “Still Face Experiment” work in 1975; his 2007 video has over 1.3 million hits. First a mother and child play in a responsive, attuned way, so the baby learns to interact with the world. Then she suddenly stops attuning. Video at: www.youtube.com/watch?v=apzXGEbZht0&feature=youtu.be
FN4 Norton Textbook Series on Interpersonal Neurobiology:
— Schore, Allan N., “The Science of the Art of Psychotherapy,” April 2012; 480 pages
— Schore, Allan N., “Affect Regulation and the Origin of the Self,” Norton textbook May 2003; first edition 1994; 432 pages
“Rider for Change” James Encinas arrived by mountain bike at San Diego’s Cherokee Point Elementary May 2 to the delight of some hundred students, and visitors from around southern California. James, a career LA school teacher, is riding 3,000 miles from Sacramento to Philadelphia. He’ll take the southern route through Texas and Louisiana, then follow the Underground Railway by which African Americans escaping slavery crossed north to freedom.
James is riding to draw national attention to the need for “trauma-informed schools,” key to the movement for “Trauma-Informed Care (TIC)” in education, health, and all public systems. But what is Trauma-Informed Care, and what’s a trauma-informed school ? (Hint: all the pix in this blog are from Cherokee Point).
“In medicine, a patient is sent to hospice when all medical procedures have failed, and they’re going to die. That says: we give care and comfort only when nothing else works,”notes Dr. Christopher Germer, psychology prof at Harvard Medical School and co-editor of Mindfulness and Psychotherapy. Pretty crazy right there, if you consider. Been in a hospital lately? Often you’re a widget; they take your clothes away, don’t tell you what’s happening, and so on. [FN1]
But when treating the real human being, “Care Equals Cure,” says Dr. Germer. If a therapist doesn’t care, he’s not going to cure his client. But it’s also true in any dealings with humans. “Care IS the practice of non-resistance to suffering which dismantles emotional suffering,” says Germer. “It means opening to emotional pain more fully, instead of trying to bypass it. Compassion opens the heart, reveals inner suffering, and makes the suffering available for transformation.” (Above: James and activists carry food donated for kids.)
“So the message is: Stop fixing,and start caring,” Dr. Germer concludes. In fact, it’s brain science. Comfort, care, compassion reduce so much of a human’s fight-flight reflex, even in major medical pain, that this has been shown to heal surgeries faster. Pain and bodily trauma create enough fight-flight that the brain stem often shuts down the immune system, for one. Compassion helps it come back online. “Let a wounded soldier talk to his mom and he’ll require 50% less pain meds,” says Dr. Bruce Perry, MD.
But could it be necessary or work well in schools?
History of Trauma-Informed Care (TIC)
TIC goes back to 1994 when the federal Substance Abuse and Mental Health Services Administration (SAMHSA) began to study the remarkably high rate of women in the mental health system with histories of physical and sexual abuse trauma. It became clear that, since such clients came in already pre-traumatized, providers should be mindful lest their own practices and policies put the women in danger, physically or emotionally, or lead to re-traumatization. (Activist Dana Brown with youth leaders.)
These and related studies next showed high rates of earlier life trauma in clients seeking services for substance abuse, domestic violence, child welfare and many other areas. In 2005 SAMSHA created the National Center for Trauma-Informed Care (NCTIC) to assist all public programs to implement Trauma-Informed Care, not only in mental health, but in all services including criminal justice and the education system. [FN 2]
“NCTIC seeks to change the paradigm from one that asks, “What’s wrong with you?” to one that asks, “What has happened to you?” says SAMHSA. “Trauma includes physical, sexual and institutional abuse, neglect, inter-generational trauma, and disasters that induce powerlessness, fear, hopelessness, and a constant state of alert…often resulting in recurring feelings of shame, guilt, rage, isolation, and disconnection.”
It’s impossible to successfully treat human beings in that condition without recognizing this and at least following the principle of “Do No Harm.” “When a program becomes trauma-informed, every part of its organization and service delivery system is assessed… to include a basic understanding of how trauma affects the life of an individual,” SAMHSA notes.
Schools are key, since all Americans are supposed to spend 13 years there. “If fixing school discipline were a political campaign, the slogan would be ‘It’s the Adults, Stupid!’,” says Jane Stevens, founder of ACEsConnection; “More than three million kids are suspended or expelled each year” in the U.S., 3.4 million in 2006 according to the National Center for Education. “But punishment doesn’t change behavior; it just drops hundreds of thousands of kids into a school to prison pipeline.” (Above: Kids ask James questions.)
“Instead of waiting for kids to behave badly then punishing them, trauma-informed schools are creating environments in which kids can succeed,” she says. It’s about re-training the adults to drop their fears and assume that kids are basically good, but something traumatized them, so they act out. Bad behavior isn’t accepted and it is corrected – by a dialog with kids to hear what’s hurting inside, and show them how to address it. “Focus on altering behavior of teachers and administrators, and kids stop fighting and acting out in class. They’re more interested in school, they’re happier and feel safer,” Stevens says. [FN3]
See the Grade or see the Person?
As SAMHSA began trauma studies in 1994, the Adverse Childhood Experiences (ACE) Study (1994-98) documented a shocker: about 50% of Americans have significant child trauma. The 17,421 HMO clients studied were privileged to be mostly college-educated, have jobs and good health care. Yet more than half had two of ten types of childhood trauma: physical abuse; sexual abuse; alcoholic or drug addict parent; family member in jail; battered mother; parent with mental illness; loss of a parent; physical neglect, emotional neglect; or verbal/emotional abuse.
The ACE Study compared their childhoods, to whether they later developed life-threatening physical conditions and/or addictions. “It found that those 10 types of severe and chronic childhood traumas up the risk of adult onset of major diseases. But it also increases the chances of being violent, a victim of violence and becoming chronically depressed,” Stevens reports in a terrific post on Cherokee Point El. “Brain research revealed one reason: the toxic stress of trauma damages the structure and function of a child’s brain. Kids get anxious and can’t sit still; get depressed and withdraw; get angry and fight; can’t focus and stop learning. They cope with anxiety, depression, anger by drinking, smoking, drugs, fighting, stealing, overeating, and/or becoming overachievers on their way to being workaholics.”
What about not-so-privileged kids? Child trauma and its mortal results must affect a far higher percentage of kids in low-income areas with less access to nutrition, health care, and on and on. A huge percentage of American children suffer trauma, bigger than 50% if we knew the real national average.
Meanwhile many of us privileged middle class kids grow up to be teachers, administrators, and so on. If we’re traumatized ourselves, we can’t feel our feelings– so we believe that considering “feelings” is idiotic. Instead, we set up schools as a place to tell kids things. Because adults talked at us, we think it’s adult to talk at kids. We tell kids they are there to listen to information and repeat it back as we want it, ie. “get the grade,” or face trouble. Enough to put anyone into fight-flight. (James Encinas, left, with students, Principal Godwin Higa, activists.)
I’m from that privileged middle class. I often say, “Nobody beat me or raped me; what’s wrong with me?”
On Feb. 25 this year, I heard Ruth Beaglehole, founder of Echo Parenting and Education, address Echo’s annual Los Angeles meeting. Urging the 150 professionals present to get passionate about raising awareness of child trauma, she said, “Kids have to live in the real world? Make the real world non-violent and trauma-sensitive! What about creating places where children can seek safety, where children can come home to people who open their arms, attune to them, and say ‘Tell me what happened today’. ” (Above: Principal Higa helps Cherokee students make origami cranes for charity.)
“Some people define that as a report card and demand, ‘I want to see your grades.’ Enough of these bloody grades!” Ruth said, to audience laughter, including mine. “Why do we accept this? Why do we accept that that’s the definition of a person — their grades?”
Suddenly out of nowhere I began violently sobbing at my table full of therapists, about 20 feet from the podium. “I see you,” Ruth said, looking straight at me. “You don’t have to hold it back.” She saw the real person I am, she didn’t need me to fake anything. She was willing to simply be with me in the pain, as Chris Germer said: “Stop fixing, start caring.” Boy did that feel good. [FN4]
I knew I always hated having to go out and get that grade, and it better be above 90 “or else.” So I did it, but I lived in fear. They didn’t see me. I was a widget who had to produce results or there’d be trouble.
Back story? On Feb. 8, 2011, I’d just heard I might have a thing called “attachment disorder.” Late one night I dragged myself to the sink to wash, listening to a CD by Dr. Henry Cloud. He joked about a lady who didn’t like her husband to go bowling: “She’s not old enough to be dropped off at school.” But it wasn’t funny. [FN5]
“That’s it: I wasn’t old enough to be dropped off at school,” I journaled, “I was just dumped off.” Terrified, I slumped in a heap sobbing, clutching a stuffed dog and a soggy toothbrush. Rising an hour later, I couldn’t even brush my teeth without holding the dog. “I’m really frightened because I don’t know if this hole under my feet ever ends,” I muttered into my pocket recorder.
I didn’t know last February but read later that Ruth was born in New Zealand to prestigious academic parents who didn’t see Ruth, either. “I baby-sat since age 12, trying to give to vulnerable children what I didn’t get,” she says. So she took a BA in early childhood ed, moved to LA, got a Masters in family therapy, and grew Echo Parenting into an agency of 23 staff that trains 100 professionals a year in service.
What if Ruth’s right? What if a school’s whole mission were to look at each child and say “I see you”? “I see you as a human being, I care how you’re feeling today, and I care what feelings and fears you’re bringing in the door. I care if you feel threatened even before you walk in the door. I want to get to know you, the real you who is. That way we can make you feel safe to be here in school. And then, you’ll really want to learn!” (One of many posters students did for James Encinas.)
———————————
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
Footnotes
FN1 Christopher Germer, PhD, “Open Heart, Open Eyes: Self-Compassion,” speech to 20th Annual Conference on Psychology of Health, Immunity and Disease, National Institute for the Clinical Application of Behavioral Medicine (NICABM), Hilton Head SC, Dec.2008
Dr. Germer [http://www.mindfulselfcompassion.org/ and http://www.centerformsc.org/ ] is a founding member of the Institute for Meditation and Psychotherapy, a clinical instructor in psychology at Harvard Medical School, author of The Mindful Path to Self-Compassion, and co-editor of Mindfulness and Psychotherapy. His meditation MP3 are here: http://www.mindfulselfcompassion.org/meditations_downloads.php “Why Self-Compassion is Becoming a Psychotherapist’s Best Between-Sessions Tool,” Dr. Chris Germer interview by Dr. Ruth Buczynski, Sept 13, 2009 is at http://www.nicabm.com/nicabmblog/can-self-compassion-become-a-portable-between-session-tool/
FN2 The Substance Abuse and Mental Health Services Administration (SAMHSA) is the agency within the U.S. Department of Health and Human Services that leads public health efforts to advance the behavioral health of the nation. Websites on TIC: http://www.samhsa.gov/nctic/ ; http://www.samhsa.gov/nctic/trauma.asp
FN3 Jane Stevens, ACEsConnection.com and ACEsTooHigh.com: http://blogs.psychcentral.com/organizations/2014/04/5-reasons-we-struggle-to-be-trauma-responsive-and-why-the-struggle-should-continue/
FN4 Ruth Beaglehole, founder of Echo Parenting and Education, address to Echo’s annual Los Angeles meeting “Developmental Trauma: Changing the Paradigm,” Feb. 25, 2014
FN5 Dr. Henry Cloud, PhD, “Character Discernment for Dummies, Part 2,” CD, Dec. 6, 2010, www.CloudTownsendResources.com
Want to heal developmental trauma in kids? Create children’s choirs, I wrote last week. Dr. Bruce Perry says “patterned, repetitive, rhythmic regulation” is what regulates the brain stem, and when it’s not regulated, we can’t truly reach the rest of a child’s brain.
The brain science studies have been done on yoga, meditation, EMDR and so on — not on Bach. But is that only because those scientists were never given the chance to sing Bach? Chalk it up to the decline of education. What if Bessel van der Kolk had sung in the Vienna Boys’ Choir? (Ok, so he’s from Holland…) Or haven’t I seen the brain science studies on choirs? Please leave me a comment!
Plus: there’s a lot of science that shows music helps shape babies in the womb — and keeps them alive when they need it. Science shows this “medical music therapy” helps people of all ages. Put this with the fact that children’s choirs have been a keystone of civilization since at least 700BC [FNO] and we start to see a pattern.
The Music in Your Cells
What we do know is that everybody loves music because every bodyloves music. Music is literally built into the human cells, especially brain cells from the hour of conception. Our bodies physically need it. Infants and children know that instinctively. “The first music encoded deep within your memory are the earliest vibrations that made you – the rhythms and tempos of your first cells,” writes Galina Mindlin, MD, Columbia University Professor of Psychiatry. [FN1]
“As your cells began to develop with the comforting rhythms of your mother’s heartbeat and the whooshing low frequency sounds vibrating through her placenta and your umbilical cord, these first musical scores began entrainment (two or more rhythms synchronizing into one) in your brain and orchestrating the essence of music for your entire being. So from your first spark of life, your brain was already establishing the relationship for how music affects you today…
“Newborns can almost immediately show some memory of sounds they encountered in the womb… Before any of us is capable of speaking words, we can recognize changes in notes and rhythmic patterns… Throughout all this development, lyrical and comforting ‘motherese,’ the singsong way in which parents speak to their children, plays a significant role in instilling feelings of calm, safety, and love…
“By only their 14th week, children can distinguish their mother’s footsteps from anyone else’s, and discriminate between their mother’s voice and a stranger’s… At the beach on any given day, we can see a man or woman lying in the sand… listening to the whoosh of waves and the easy hush of wind, smiling like a baby…”
“Music in its most primodial form links our brain to vibrations we experienced as babies that have both long- and short-term effect on our brains’ circuitry. The core characteristics of music – rhythm, harmony, synchrony, resonance, and dissonance – can affect frequencies in our brain and extend their influence on our hormones, neurotransmitters, and essential enzymes, and can ultimately affect our focus, feelings, moods, motivation” and more. [FN2]
Music Therapy Saves Preemies
Dr. Joanne Loewy, Director of the Louis Armstrong Center for Music and Medicine at New York’s Beth Israel Hospital, saves lives of premature babies (and other patients) using music to replicate the auditory environment in the womb. I haven’t asked Dr. Loewy about choirs, but to me this work says worlds about what singing can do to regulate the physiology and thus the brains of kids. Dr. Loewy sings to a newborn, above. [FN 3]
I first met Dr. Loewy by email shortly after the Beth Israel team she heads published a major study on medical music therapy for preemies on April 15, 2013. First off, I was blown away to learn there exists a Louis Armstrong Center for Music and Medicine at the top hospital in New York City. It’s official: music is essential to humans! [FN4]
I was also delighted when she invited me to see her for music therapy to heal my pre-concious anxieties from being an unwanted pregnancy. Gosh, she trains music therapists worldwide and teaches at the Albert Einstein College of Medicine. It was too long a commute from California. But I started music therapy anyway and it sure works for me.
“By re-creating a womb-like environment through sound and music, music therapy has been shown to deepen infant sleep-state, support infant self-regulation, assist in the stabilization of breathing and heart rates, enhance parent/infant bonding, sooth irritability, re-enforce feeding/sucking rhythms and weight gain, and promote a sense of safety during painful procedures” faced by many preemies,” she wrote.
“Historically, we thought premature infants were best left alone in a quiet, closed incubator with no stimulation,” she told the press when the study came out. “But more recently, we’re seeing that the right kind of stimulation — particularly live, interactive music — can enhance babies’ neurological function and increase their quiet-alert state. . . . the more we can regulate the sound environment, the better they’re going to fare.” [FN 5]
Dr. Loewy’s team studied 272 infants in 11 hospital neonatal intensive care units (NICUs). They found that live music matched to babies’ breathing and heart rates enhanced feeding and sleeping patterns. Parent-selected lullabies also seemed to promote bonding between parents and babies, easing the stress of the chaotic NICU environment.
The music also lowered parental stress, the study found — which is key, because anxious, fearful, clueless parents produce developmental trauma in their kids. Parent-preferred melodies and entrained live rhythm and breath sounds enhanced quiet alert and sleep states, suck response, and oxygen saturation in premature infants and also significantly reduce fear and anxiety perception in parents, they found.
Over two weeks, the 272 premature babies underwent several sessions of two instruments, singing and no music at all. The instruments and lullaby singing style were intended to approximate womb sounds, said Dr. Loewy. Two-tone heartbeat rhythms were played on a “gato box,” a rectangular wooden drum. [Bruce Perry and Bessel van der Kolk speak extensively on the primacy of the mother’s heart rate in determining fetal brain development. Dr. van der Kolk strongly recommends heart-rate variability regulating therapies for trauma. -kb]
Whooshing sounds [like those in the womb referenced by Dr. Mindlin and I suspect by numerous researchers] were produced by an “ocean disc,” a cylinder containing shifting metal beads.
For melody, parents were asked for a favorite song. If it wasn’t a lullaby (one chose “I Heard It Through the Grapevine”; another, “Pick Up the Pieces”), therapists slowed it, changed meters to lullaby-like waltzes and adjusted lyrics.
“Lots of times you see parents bopping the baby up and down on their lap, and there’s no purpose to it,” Dr. Loewy said. “You don’t feel the music intention as much as if you have a song that a parent has chosen.” If parents did not specify, researchers used “Twinkle, Twinkle, Little Star.” Tempos were coordinated with babies’ vital signs, indicated not only by monitors but also by baby eye movements and its chest’s rise and fall.
Researchers found that the heart beat gato box, the whooshing ocean disc and the singing, all slowed a baby’s heart rate, though singing seemed most effective. Singing also increased the time babies stayed quietly alert. Sucking behavior improved most with the gato box. Breathing rate slowed most and sleeping was best with the ocean disc. Babies hearing songs their parents chose had better feeding behavior and gained more calories than those who heard “Twinkle, Twinkle, Little Star.” But the “Twinkle” babies had slightly more oxygen saturation in their blood.
“Many NICUs are noisy, or people put on random lullabies that are recorded,” Loewy said. “But it’s not just any recorded lullaby, it’s the power of the parent’s voice synchronized therapeutically . . . and the other two sounds can have a therapeutic benefit.”
———————————
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
Footnotes
FNO Chorus members in Greek theater were trained in childhood from around 700 BC. Greek theater always included a chorus, whose members also danced and spoke, but also sang: http://en.wikipedia.org/wiki/Greek_chorus Both boys and girls were trained to sing: http://www.amazon.com/Choruses-Young-Women-Ancient-Greece/dp/0742515249
Greece and Rome founded many children’s singing schools: http://www.boychoirs.org/library/history/hist014.html
The Schola Cantorum in Rome was formed in the seventh century to train boys in reading and singing.
FN1 Galina Mindlin, M.D., Ph.D is Assistant Clinical Professor of Psychiatry at Columbia University College of Physicians and Surgeons, and Supervising Attending Physician at the Department of Psychiatry in St. Luke’s Roosevelt Hospital Center. She is Board Certified in psychiatry and neurology. See also: www.nicabm.com/nicabmblog/what-healthy-brains-sound-like-how-brain-music-therapy-is-helping-first-responders/
FN2 Mindlin, Galina MD, PhD, “Your Playlist Can Change Your Life: 10 Proven Ways Your Favorite Music Can Revolutionize Your Health, Memory, Organization, Alertness,” Sourcebooks, Inc., Naperville, IL, 2012
FN3 Joanne V. Loewy, DA, LCAT, MT-BC, is Director,
Louis Armstrong Center for Music & Medicine,
Beth Israel Medical Center, New York, NY Websites:
http://www.musicandmedicine.org/ and http://www.facebook.com/ArmstrongMusicandMedicine
She is also Co-Editor-in-Chief, “Music and Medicine” www.sagepub.com/journals/Journal201929
FN4 “The Effects of Music Therapy on Vital Signs, Feeding, and Sleep in Premature Infants,” Joanne Loewy, Kristen Stewart, Ann-Marie Dassler, Aimee Telsey, Peter Homel
Online April 15, 2013; hard copy in May 2013 Pediatrics.
Abstract: http://pediatrics.aappublications.org/content/early/2013/04/10/peds.2012-1367.abstract
Full Text in PDF: http://pediatrics.aappublications.org/content/131/5/902.full.pdf+html
SUMMARY:
What’s Known on This Subject:
Recorded music, parent voices, and sung lullabies have been shown to increase oxygen saturation, nonnutritive sucking, and weight gain in premature infants.
What This Study Adds:
Parent-preferred melodies and entrained live rhythm and breath sounds can enhance quiet alert and sleep states, suck response, and oxygen saturation in premature infants and significantly reduce fear and anxiety perception in parents.
FN5 Pam Belluck, “Live Music’s Charms, Soothing Premature Hearts – Preemies and Sound,” New York Times, April 15, 2013, www.nytimes.com/2013/04/15/health/live-music-soothes-premature-babies-a-new-study-finds.html?_r=0 Maureen Salamon, “Lullabies Soothe Preemies, Parents Alike,” Philadelphia Inquirer, April 15, 2013 [webpage removed]
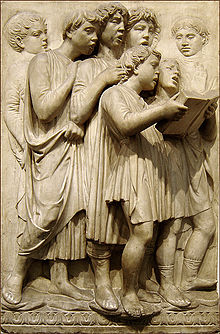
What’s that got to do with this sculpture of children singing in the Cathedral of Florence in 1436 to kick off the Renaissance? Everything!
Dr. Perry says it’s brain science to regulate the brain stem with “patterned, repetitive, rhythmic regulation,” featuring yoga, meditation, deep breathing, and singing, principles so fundamental they go back to the dawn of man. [FN1]
Who can imagine life without singing? In every culture, long before writing, the only way to pass down an idea was to sing it. Aryans have sung Vedas since 5,000 BC or before. Hebrews sang Psalms as far back as 2,500 BC, long before they were written down ca. 1400 BC. [FN2 ]
Want to regulate kids? Teach them to sing! Gathering children to sing in choirs was the core of the Greek educational system since at least 700 BC, and there were choir schools for kids in Europe at least since the 900s AD. [FN3] Singing in choirs brings kids into organized personal connection with other living, regularly-breathing human beings. Being connected and in harmony with other humans is what best regulates human beings – today brain scientists call it “limbic resonance.” [FN4]
She did it without any training. Amira just went on the internet looking for songs, found this Italian aria, and learned it by imitating. Clearly she found a terrific adult soprano – we can hear the inflections of a highly-experienced adult in Amira’s voice. [FN5]
Or take the St. Thomas Boys Choir of Leipzig. When J.S. Bach became music director in 1723, the choir school was already 511 years old. Click here for the boys singing a Bach “Gloria.” [FN6]
Born to Sing
If a child can speak, he can sing; most kids can sing before they can speak. Training children to sing as young as possible is a principle of civilization. Electronic culture has forgotten it to our peril as our kids whack out on machine-made noise. We need a revolutionary approach as old as the hills. We need children’s choirs on a mass scale.
These children singing on the “Cantoria” by Lucca della Robbia, sculpted 1431-36, were placed in the Cathedral as public ads, to urge parents to bring in their kids for training. This is the level of culture and education which later produced Bach, Haydn, Schubert and Beethoven. Was their genius just magic? Why don’t we have composers today, who produce music on such a scale (and they did it all without electronic equipment) ?
Answer: Bach & co. were trained as children to sing harmonic, complex polyphony (4-6 different musical lines at once). So complex, harmonic music was what they heard in their heads as little kids. They were bilingual; music was their second mother tongue. To them, it was simple: as soon as they could hold a pen, they would just start to write down their musical ideas. That tradition continued in Europe until the end of the 19th Century.
And there’s another reason everybody loves music: it’s because every bodyloves music. Music is literally built into kids’ bodies from the hour of conception. Our bodies physically need it. And kids know that instinctively, from infancy.
“The first music encoded deep within your memory are the earliest vibrations that made you – the rhythms and tempos of your first cells,” writes Galina Mindlin, MD and music therapist.
“As your cells began to develop with the rhythms of your mother’s heartbeat and the whooshing sounds vibrating through her placenta and your umbilical cord, these first musical scores began entraining (two or more rhythms synchronizing into one) in your brain… your brain was already establishing the relationship for how music affects you today… Newborns can almost immediately show some memory of sounds they encountered in the womb… Before any of us is capable of speaking words, we can recognize changes in notes and rhythmic patterns…” [FN7]
The Mother of All Trauma
What about trauma healing? Consider this: from 1348-1350, the Black Death, the mother of all trauma, killed half the population of Asia and Europe. In Italy, Florence’s population was reduced from 120,000 in 1338 to 50,000 in 1351. Many thought civilization was finished. [FN8]
Then a handful of intellectuals devised the idea of a re-birth or “Renaissance,” a project to unite a new economics to feed the population, with the science, philosophy, and arts to uplift them. Florence had a famous problem whose solution could inspire people with hope. At the city’s center lay the massive Cathedral of Florence, begun 1296 — but no one had any idea how a dome could be built large enough to cover such a space without collapsing. Work was also delayed by waves of plague for decades. The roof lay open for over a century as people prayed in the rain.
During 1402–1404, Filippo Brunelleschi and his friend Donatello visited Rome to study the ancient ruins and the Pantheon on which the Cathedral was modeled. They returned to build the first “classical” buildings in Florence. In 1420, Florentine banker Cosimo de’ Medici (1389-1464) bankrolled Brunelleschi to work 16 years to complete the first octagonal dome in history to be built without a wooden supporting frame. [FN9]
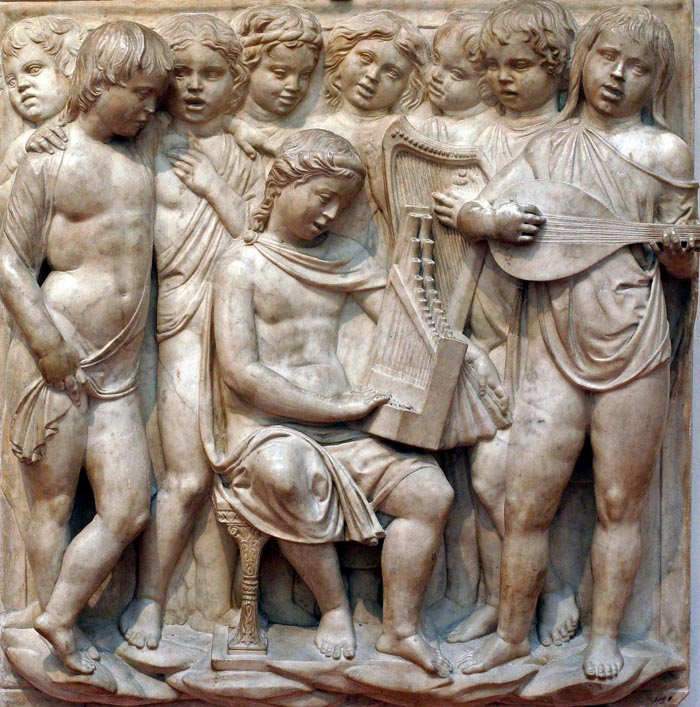
What did they do in that Cathedral? They brought in the children of the city and taught them to sing, to show there was hope for the future, that the children could be saved from the jaws of death. These sculptures just above show that by the age of 9-11, kids were singing (and playing) complex four and six part polyphony.
Note the rounded mouths in all the sculptures (and in the St. Thomas boys). Vocal scholars can tell you what note they’re singing by how large of an egg-shaped mouth they’re making.
The dome was ready in time for the Council of Florence which opened in the Cathedral on March 25, 1436, the date often cited as the start of the Renaissance. Inside were featured these sculptures of children singing in the choir loft by Lucca della Robbia. Flemish composer Guillaume Dufay and many of his colleagues were brought to Italy to teach advanced musical composition. Dufay’s advanced motetNuper rosarum flores was composed for the 1436 opening and sung from della Robbia’s choir loft by kids like these in the sculptures.
Cosimo de’ Medici and his grandson Lorenzo de’ Medici (1449-1492) also backed philosophers Marsilio Ficino and Pico della Mirandola. Pico’s 1486 “Oration on the Dignity of Man” stated the Renaissance Idea: each individual human soul is a divine spark of God, not a beast of burden as under feudalism.
These sculptures show that in Florence, the Dignity of Man began with the dignity of the children. These kids have been taught to sing even younger, at 5 to 8 years. Della Robbia did several sculptures of toddlers singing as well (more than I have space to show!).
Even infants sang, singing with their families perhaps while they learned to speak.This child is not much older than 2. Kids who started this early acquired the experience it took to produce genius in many fields.
San Diego Trauma-Informed Renaissance?
I’ve seen this kind of singing of fine music in choirs make traumatized children happy. Musicians who run children’s choirs will tell you that.
The San Diego Children’s Choir (right), founded 1990, now has 5 branches with over 250 participants. It also has a neighborhood outreach program that spans many low-income areas full of traumatized children including City Heights and other areas.
City Heights is also where Principal Godwin Higa has been turning Cherokee Point Elementary into an advanced trauma-infomed school since 2008. Three professors at San Diego State and community organizers Dana Brown and Dorothy Zirkle worked with the City Heights community to develop a two-year $684,094 pilot project at Cherokee Point, the Wellness and Restorative Practice Partnership (WRPP), funded by the California Endowment.
I can’t be with Bruce Perry in Washington May 4, but I will be in San Diego May 2, talking to my friend Dana Brown and other members of the San Diego Trauma-Informed Guide Team (SD-TIGT) about Bruce Perry, Bessel van der Kolk, and the brain science of trauma. SD-TIGT is leading the way among county health and welfare institutions to implement trauma-prevention and trauma-healing practices in schools, medical, and social facilities.
If Principal Higa and Dana haven’t met the folks at the San Diego Children’s Choir yet, maybe I’ll be able to provoke something. Even if they’ve met, maybe we can expand their forces. As a result of the economic crisis, San Diego just lost its opera company, the San Diego Opera. The city must be full of struggling singers, school music teachers and private voice teachers who would jump at the chance to teach every child at Cherokee El to sing Bach.
Next step: find our Cosimo de’ Medici to pay these already financially-pressed musicians and educators, so they can put in the hours necessary every week at Cherokee El. Then stand back.
FN1 Lucca della Robbia, Cantoria (Choir Loft), shows children singing, dancing,and making music to “praise the Lord” in the words of Psalm 150. Photos at http://commons.wikimedia.org/wiki/File:Cantoria_di_luca_della_robbia_11.jpg
FN3 Chorus members in Greek theater were trained in childhood from around 700 BC. Greek theater always included a chorus, whose members also danced and spoke, but also sang. [http://en.wikipedia.org/wiki/Greek_chorus ] Both boys and girls were trained to sing. [http://www.amazon.com/Choruses-Young-Women-Ancient-Greece/dp/0742515249 ] Greece and Rome founded many children’s singing schools [ http://www.boychoirs.org/library/history/hist014.html ] The Schola Cantorum in Rome was formed in the seventh century to train boys in reading and singing.
The Vienna Boys Choir, formalized in a 1498 letter by Maximilian I Habsburg, goes back to the year 957 when Bishop Wolfgang of Regensburg created his cathedral choir [ http://www.boychoirs.org/library/history/hist014.html and http://en.wikipedia.org/wiki/Vienna_Boys%27_Choir ] The first choir school was founded at St. Paul’s Cathedral, London in 1127, the second at St. Thomas’ Church, Leipzig in 1212. A boarding school for choristers at the Kreuzkirche in Dresden is mentioned in 1300, a choir known now as the Dresdner Kreuzchor. The Vienna Boys Choir received a solid musical education, many went on to become professional musicians such as Franz Schubert.
[ http://en.wikipedia.org/wiki/Choir ].
FN4 Lewis, Thomas, MD; Amini, Fari, MD; Lannon, Richard, MD; “A General Theory of Love”, Random House, New York, 2000. Lannon interviews : www.paulagordon.com/shows/lannon/
FN7 Mindlin, Galina, MD, PhD, “Your Playlist Can Change Your Life,” Sourcebooks, Inc., Naperville, IL, 2012 More here:
www.nicabm.com/nicabmblog/what-healthy-brains-sound-like-how-brain-music-therapy-is-helping-first-responders/
FN8 The Black Death was one of the most devastating pandemics in human history, peaking in Europe between 1348 and 1350 with 30–60 percent of Europe’s population killed. It reduced world population from an estimated 450 million to between 350 and 375 million in the 14th century. http://en.wikipedia.org/wiki/Consequences_of_the_Black_Death
FN9 Walker, Paul Robert, “The Feud That Sparked the Renaissance: How Brunelleschi and Ghiberti Changed the Art World,” Harper Collins, 2003
Dr. Bruce Perry, MD is taking his healing for trauma to Washington in a May 4 program for the National Council for Behavioral Health.
And the doc’s got rhythm. In fact, he and other trauma experts are reporting revolutionary success with treatments using yoga, meditation, deep breathing, singing, dancing, drumming and more.
These principles are so fundamental to our brains they go back to the dawn of man; the Vedas were sung before 5,000 BC (likely with yoga and meditation.) My book describes how yogic chant and meditation saved my life in 2010, before I ever read a word about brain science.
One California county is trying to cancel such programs, insisting on Cognitive Behavioral Therapy (CBT) which relies on the thinking brain. But Perry and many experts say talk therapy alone can re-traumatize trauma survivors.
Perry says we need “patterned, repetitive, rhythmic somatosensory activity,” literally, bodily sensing exercises. Developmental trauma happens in the body, where pre-conscious “implicit memory” was laid down in the primitive brain stem (survival brain) and viscera. Long before we had a thinking frontal cortex or “explicit memory” function. [FN1]
The list of repetitive, rhythmic regulations used for trauma by Dr. Perry, Dr. Bessel van der Kolk, Dr. Pat Ogden and others is remarkable. It includes singing, dancing, drumming, and most musical activities. It also relies on meditation, yoga, Tai Chi, and Qi Gong, along with theater groups, walking, running, swinging, trampoline work, massage, equine grooming and other animal-assisted therapy…. even skateboarding. Click here for Perry’s web page on interventions.
“I am asked how hip hop and skateboarding can help a child with depression or ADHD,” reports Dr. Sarah MacArthur of the San Diego Center for Children. “Yet 70% of the children showed improvement in symptoms of depression, anxiety, and PTSD.” [FN2]
The Brain Stem Rules
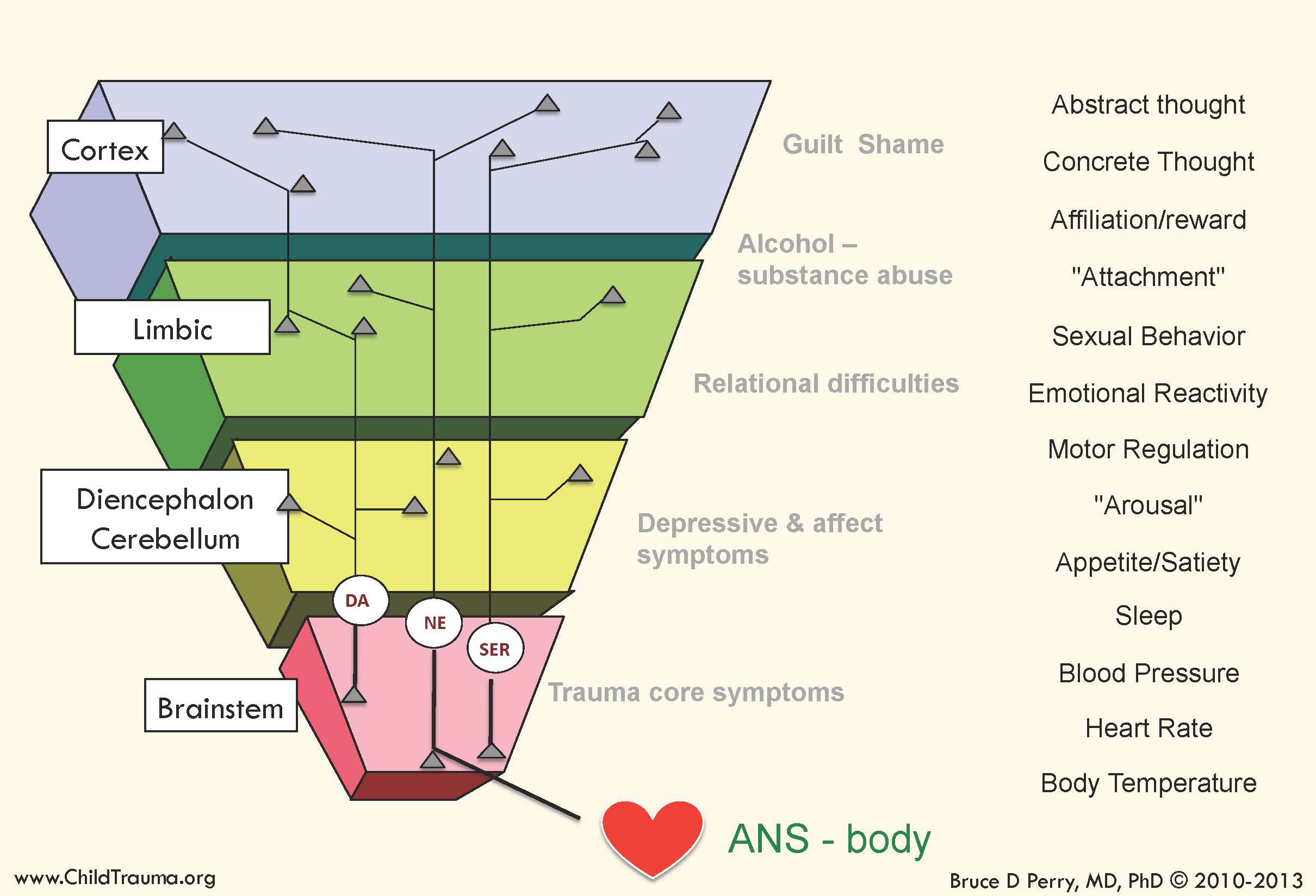
“The brain organizes from bottom to top, with the lower parts of the brain (brain stem/diencephalon aka “survival brain”) developing earliest, the cortical areas (thinking brain) much later,” Perry says. “The majority of brain organization takes place in the first four years.
“Because this is the time when the brain makes the majority of its “primary” associations… early developmental trauma and neglect have disproportionate influence on brain organization and later brain functioning… When a child has experienced chronic threats, the brain exists in a persisting state of fear… and the lower parts of the brain house maladaptive, influential, and terrifying pre-conscious memories… ” [FN3]
“People with developmental trauma can start to feel so threatened that they get into a fight-flight alarm state, and the higher parts of the brain shut down,” says Perry. “First the stress chemicals shut down their frontal cortex (thinking brain). Now they physically can not think. Ask them to think and you only make them more anxious.
“Next the emotional brain (limbic brain) shuts down. They have attachment trauma, so people per se seem threatening; they don’t get reward from emotional or relational interaction.
“The only part of the brain left functioning is the most primitive: the brain stem and diencephalon cerebellum. If you want a person to use relational reward, or cortical thought – first those lowest parts of the brain have got to be regulated,” Perry concludes.
“We must regulate people, before we can possibly persuade them with a cognitive argument or compel them with an emotional affect.
“The only way to move from these super-high anxiety states, to calmer more cognitive states, is rhythm,” he says. “Patterned, repetitive rhythmic activity: walking, running, dancing, singing, repetitive meditative breathing – you use brain stem-related somatosensory networks which make your brain accessible to relational (limbic brain) reward and cortical thinking.
“Cognitive behavioral therapy (CBT) is great if you have a developed frontal cortex – but we’re talking about a five year old kid who’s so scared to death most of the time that it’s shut down his frontal cortex ’cause he just saw his mother get shot,” Perry told an audience of therapists. “You’re going to do 20 sessions of CBT and expect change? That’s a fantasy.” [FN4]
6 R’s for Healing Trauma
Dr. Perry does separate developmental “maps” of each person (left) using his “Neurosequential Model of Therapeutics” (NMT). Each individual is so unique that using NMT needs training; this blog is meant only to point you toward it. For an overview of NMT, click here for Perry, B.D. and Hambrick, E. (2008), “Neurosequential Model of Therapeutics.“ Click here for training in NMT and Somatosensory Regulation.
Trauma healing, says Perry, requires 6 R’s; it must be:
• Relational (safe)
• Relevant (developmentally-matched to the individual)
• Repetitive (patterned)
• Rewarding (pleasurable)
• Rhythmic (resonant with neural patterns)
• Respectful (of the child, family, and culture)
“To change any neural network in the brain, we need to provide patterned, repetitive input to reach poorly organized neural networks involved in the stress response. Any neural network that is activated in a repetitive way will change,” Perry explains.
“The rhythm of these experiences matter. The brain stem and diencephalon contain powerful associations to rhythmic somatosensory activity created in utero and reinforced in early in life. The brain makes associations between patterns of neural activity that co-occur.
“One of the most powerful sets of associations created in utero is the association between patterned repetitive rhythmic activity from maternal heart rate, and all the neural patterns of activity associated with not being hungry, not been thirsty, and feeling ‘safe’ (in the womb).
“Patterned, repetitive, rhythmic somatosensory activity… elicits a sensation of safety. Rhythm is regulating. All cultures have some form of patterned, repetitive rhythmic activity as part of their healing and mourning rituals — dancing, drumming, and swaying.
“EMDR and bilateral tapping are variations of this patterned, repetitive rhythmic, somatosensory activity… We believe that they are regulating in part because they are tapping into the deeply ingrained, powerful permeating associations created in utero.” [FN5]
For each child, the NMT develops a unique, personalized “map” (see above) of what the specific neurological damage has been, how far development has come (or not), and where the child needs to go. Next it creates “a unique sequence of developmentally-appropriate interventions,” says Perry. “While many deficits may be present, the sequence in which these are addressed is important. The more the therapeutic process can replicate the normal sequential process of development, the more effective…
“The first step in therapeutic success is brain stem regulation… Start with the lowest undeveloped/ abnormally functioning set of problems and move sequentially up the brain as improvements are seen…
“An example of a repetitive intervention is positive, nurturing interactions with trustworthy peers, teachers, and caregiver… using patterned, repetitive somatosensory activities such as dance, music, movement, yoga, drumming or therapeutic massage… This is true especially for children whose persisting fear state is so overwhelming that they cannot improve via increased positive relationships, or even therapeutic relationships, until their brain stem is regulated by safe, predictable, repetitive sensory input.” [FN6]
Sound like your family doctor saying “Go calm down in the gym” ? I thought so – until I tried it. It works, big time. My story is here: “Dr. Perry: Music Makes Your Case.”
———————————
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
Footnotes
FN1 Perry, Bruce D., MD, “Born for Love: The Effects of Empathy on the Developing Brain,” Annual Interpersonal Neurobiology Conference “How People Change: Relationship & Neuroplasticity in Psychotherapy,” UCLA, Los Angeles, March 8, 2013 (unpublished).
Library of articles on interventions, trauma, brain development: https://childtrauma.org/cta-library/
Training in NMT Method and Somatosensory Regulation, Power of Rhythm — Individual and Site Training Certification Programs, DVD/streaming training, and online training: http://www.ctaproducts.org
Dr. Perry’s latest research and key slides: “Helping Children Recover from Trauma,” National Council LIVE, National Council on Behavioral Health, Sept. 5, 2013 at www.thenationalcouncil.org/events-and-training/webinars/webinar-archive/ (scroll down to Sept. 2013.)
Dr. Perry’s YouTube channel with educational videos in depth: https://www.youtube.com/channel/UCf4ZUgIXyxRcUNLuhimA5mA?feature=watch
FN3 Perry, B.D. and Hambrick, E. (2008), “The Neurosequential Model of Therapeutics (NMT),” Reclaiming Children and Youth, 17 (3) 38-43; and Dobson, C. & Perry, B.D. (2010), “The role of healthy relational interactions in buffering the impact of childhood trauma in “Working with Children to Heal Interpersonal Trauma: The Power of Play,” (E. Gil, Ed.), The Guilford Press, New York, pp. 26-43
Both at: http://childtrauma.org/nmt-model/references/
FN4 Perry, Bruce D., “Born for Love,” op. cit. FN1
FN5 MacKinnon, L. (2012), “Neurosequential Model of Therapeutics: Interview with Bruce Perry,” The Australian & New Zealand Journal of Family Therapy, 33:3 pp 210-218, http://childtrauma.org/cta-library/interventions/
Dr. Bruce Perry, MD (left) documents the brain science of how attachment problems can cause developmental trauma to a fetus, infant, or child – just when the brain is developing.
And he’s taking his “attachment first” approach to Washington. In “Trauma Impacts the Brain: Healing Happens in Relationships,” Perry leads a full-day Pre-conference University on Sunday May 4, to kick off the National Council for Behavioral Health’s Annual Conference ’14 on May 5-7 (click here for details).
“Experiences profoundly influence the development of young children. Adverse Childhood Experiences (ACEs) shape the brain’s organization, which, in turn, influences the emotional, social, cognitive, and physiological activities,” the conference website notes.
“So often, trauma happens in relationships, but it is also in relationships that healing occurs. Explore the latest research and clinical treatment with trauma researcher, treatment visionary, and bestselling author of The Boy Who Was Raised as a Dog, and Born for Love: Why Empathy is Essential and Endangered, Dr. Bruce Perry.”
Dr. Perry’s relationship and attachment theory healing model first assesses each child as an individual, using his Neurosequential Model of Therapeutics (NMT). He emphasizes that there is no one label for child trauma. Rather, “there are very individualized patterns of exposure to trauma (all with unique timing, nature, and patterns)… So we don’t call ‘it’ anything,” he wrote me recently. “We describe it — and try to ‘illustrate’ each individual’s trajectory separately” with the NMT’s individualized brain mapping technique. [FN1]
Dr. Perry recommends his books above as the best summaries of his work. His latest research and key slides are online from his National Council webinar last fall, “Helping Children Recover from Trauma,” National Council LIVE, Sept. 5, 2013 (scroll down to Sept. 2013.) I really recommend this – and it will only be online through August 2014.
Dr. Perry says we’ve got to learn about the neuro-biological growth of the brain in order of time sequence from conception to later development in infancy and childhood.
His “Four Part Brain” slide (above) shows the time sequence from the bottom up: first the brain stem develops (pink); then the diencephalon cerebellum (yellow); they make up our primitive reptilian “survival” brain. Next develop the emotional limbic brain which only mammals have (green), and finally the thinking brain aka frontal cortex (blue).
The fetus’ “survival brain” develop first, because infants require breathing, heart beat, and other survival functions at birth, Dr. Perry told a March 2013 UCLA conference. The rest of the brain develops largely after birth and as an outgrowth of the brain stem. [FN3]
So injury during brain stem development in the first 45 months harms development of the entire brain, the neurons around the viscera, and most of the body.
Dr. Perry next details three key threats to an infant’s developing brain: Trauma in utero (intra-uterine insult); post-birth attachment trauma; and other post-natal trauma – all before the thinking brain comes on line around age 3.
A fetus in utero is designed to develop in nurturing oxcytocin and other “reward” chemicals released by a mother supported by her family, all joyous a baby is coming. Intra-uterine insult occurs when the mother instead uses substances, or is under stress so that her stress hormones impact the fetus’ developing brain. This can be visible stress to the mother: domestic abuse, work stress, violence.
A fetus, however, can also be subject to stress chemicals with no visible external stress to the mother, as in mothers who are anxious, themselves victims of attachment disorder, don’t want a baby, etc. Often these mothers have no steady pattern to their heart rate, and since a baby’s brain grows according to the mother’s heart rate rhythm, the baby’s brain develops dysregulated.
All these “causes a cascade of mental and physical problems in every part of the body and brain,” Perry says. “Every part of the whole brain these neurons enervate will be dysregulated.”
Birth: the Mother of All Stress
Attachment trauma occurs easily because birth is incredibly stressful to a baby: suddenly there’s lack of oxygen, blinding light, shocking cold, terrifying noise, and pain. This floods a baby with stress hormones — which is essential because now it’s not having needs met as in the womb; thus it’s got to protest so someone comes. “If animals in the wild didn’t feel the stress of hunger they’d just lie around and die of starvation,” Perry notes.
If all goes as designed, an attuned mother meets the baby’s needs, feeds it, swaddles it, turns down the lights, so the baby feels safe and is flooded with reward optiates like oxytocin. If animals didn’t feel opiate rewards when they get up and eat just what they need (not dirt, for example), they’d not get up.
Then they wouldn’t survive, so the stress hormones and the reward opiates are linked. “At the relief of hungry-thirsty-cold stress, we feel pleasure,” Dr. Perry says. An attuned mother “has a well-organized neurobiology to create a healthy organized neural network for the infant of attachment and regulation…
“And in the arms of that caregiver, that is that magic moment literally weaving together the neurobiology of all these different systems. The biology of attachment is that a baby learns by thousands of good experiences that this stress is tolerable because it leads to reward, and this pleasurable outcome is cathexsized to a person, Mom… Ultimately just seeing or hearing Mom makes you feel safe and pleasurable. Let a wounded soldier talk to his mom, he’ll need 45% less pain meds.”
Or not.
If mom instead is under too much stress herself to meet needs, has too many children and no support, or herself was raised by a mis-attuned mom, “she doesn’t get reward from responding to her baby’s distress,” Perry continues. “So the pull to respond isn’t there.”
Even if no stress to the mother is visible, “if she merely meets physical needs, without involving her own pleasure systems, then the weaving together of meeting needs and the reward/safety system is weak or absent. So her baby learns that stress can be life-threatening, that stress is terrifying,” Dr. Perry concludes. [FN3 op. cit.]
The “Or Not” baby’s brain learns: “that’s all she wrote.”
It develops in a state of perpetual stress in which the stress chemicals simply do not stop and the reward chemicals never or seldom come. In this state, fight/flight cortisol flood eventually leads to “freeze” dissociation, Judith Herman reported back in 1992. [FN4]
——————————— Medical Disclaimer:This website is for general information purposes only. It is simply my own research. Individuals should always see their health care provider or licensed psychotherapist before doing anything which they believe to be suggested or indicated herein. Any application of the material on this website is at the reader’s discretion and is the reader’s sole responsibility.
Commentsare encouraged with the usual exceptions; rants, political speeches, off-color language, etc. are unlikely to post. Starting 8-22-16, software will limit comments to 1030 characters (2 long paragraphs) a while, until we get new software to take longer comments again.
Footnotes
FN1 Perry, B.D. and Hambrick, E. (2008), “The Neurosequential Model of Therapeutics (NMT),” in Reclaiming Children and Youth, 17 (3) 38-43; and Dobson, C. & Perry, B.D. (2010), “The role of healthy relational interactions in buffering the impact of childhood trauma in “Working with Children to Heal Interpersonal Trauma: The Power of Play,” (E. Gil, Ed.) The Guilford Press, New York, pp. 26-43
Both at: http://childtrauma.org/nmt-model/references/
FN2 Bruce Perry MD, Daniel Siegel MD, et.al, “Trauma, Brain & Relationship: Helping Children Heal,” www.youtube.com/watch?v=jYyEEMlMMb0 – introductory video on Attachment Disorder and development trauma. Copies at www.postinstitute.com/dvds.
FN3 Perry, Bruce D., MD, “Born for Love: The Effects of Empathy on the Developing Brain,” Annual Interpersonal Neurobiology Conference “How People Change: Relationship & Neuroplasticity in Psychotherapy,” UCLA, Los Angeles, March 8, 2013 (unpublished).
Library of articles on interventions, trauma, brain development: https://childtrauma.org/cta-library/
Training in NMT Method and Somatosensory Regulation, Power of Rhythm — Individual and Site Training Certification Programs, DVD/streaming training, and online training: http://www.ctaproducts.org
Dr. Perry’s latest research and key slides: “Helping Children Recover from Trauma,” National Council LIVE, National Council on Behavioral Health, Sept. 5, 2013 at www.thenationalcouncil.org/events-and-training/webinars/webinar-archive/ (scroll down to Sept. 2013.)
Dr. Perry’s YouTube channel with educational videos in depth: https://www.youtube.com/channel/UCf4ZUgIXyxRcUNLuhimA5mA?feature=watch
FN4 Herman, Judith, “Trauma and Recovery,” Basic Books, New York, 1992
Developmental Trauma:
What you can’t see, canhurt you.
Dr. Bessel van der Kolk, MD (left) and leaders in brain science and attachment are calling for a hard look at developmental trauma. Developmental Trauma Disorder (DTD) was identified by van der Kolk in 2005, but the psychiatric Powers That Be deny it exists. [FN1]
“Clearly our field would like to ignore social realities,” Dr. van der Kolk said recently, “and study genes…”
He’s also shown it’s at the root of borderline personality disorder and bipolar disorder, and implies it’s at the root of most cases mis-diagnosed as ADHD/ADD. See his terrific May 10, 2013 speech at Yale: Youtube.com/watch?v=N2NTADxDuhA
I dubbed it “trauma since the sperm hit the egg” when I realized I had it. Dr. Allan Schore calls it “trauma in the first 1000 days, conception to age two.” It used to be called “complex PTSD” (C-PTSD) or “Early Trauma” (ET).
Developmental trauma starts in utero when we don’t have much more than a brain stem, and goes on during the pre-conscious years. It can continue until 24 or 36 months depending on when the thinking brain (frontal cortex) comes on line. That’s up to 45 months living in general anxiety to non-stop terror — before age 3. A very long time to an infant.
DTD occurs as a continual process, not discrete incidents, while a baby has not developed a thinking brain able to recall incidents. Frequently it occurs before there are any discrete incidents.
“No one can see it” means “it never happened.” As I’ve said, “No one beat me or raped me. What’s wrong with me?” Try getting that treated.
Neuroscientists Dr. Daniel Siegel, MD, Dr. Bruce Perry MD and others detail how attachment failures cause developmental trauma in this video: www.youtube.com/watch?v=jYyEEMlMMb0 [FN2]
Insecure Attachment as the Cause
DTD is a “Relational Trauma, trauma in the context of a relationship” as Dr. Allan Schore (left), father of attachment theory in the U.S., identified it in the 1990s. [FN3] Only relational processes can explain DTD, not incidents.
Yet all the American Psychiatric Association (APA) can fathom is Post-Traumatic Stress Disorder (PTSD) — since it’s caused by a visible incident such as war injury or rape. Developmental trauma has no incident. It’s ingrained in brain and visceral tissue, with no obvious “big bang,” so some call it “little ‘t’ trauma,” as opposed to visible PTSD “Big ‘T’ Trauma.”
Insecure attachment and attachment disorder generally are the cause of developmental trauma, not vice versa, Dr. van der Kolk detailed in his May 2005 Psychiatric Annals pdf noted above and in FN1. He emphasized it again at Yale on May 10, 2013 (video link above). He lists DTD’s symptoms as relational and chronic: inability to concentrate or regulate feelings; chronic anger, fear and anxiety; self-loathing; aggression; and self-destructive behavior. [FN4A]
Working with the National Center for Child Traumatic Stress Complex Trauma Network (NCTSN), van der Kolk reports that he ran a survey of 40,000 children nationally being treated for multiple traumas. Most of them “do not meet the criteria for PTSD… (as) the majority of issues are not specific traumas, but issues in their attachment relationships,” he says.
Van der Kolk describes studies by his colleague Dr. Marylene Cloitre, on attachment problems as the cause of DTD. “Marylene looked at chronic complex trauma symptoms, then she did child attachment interviews, Dr. Mary Main’s interviews, in which I hope all of you have been trained, because they are very very helpful to see what were peoples’ experiences of their childhoods,” he said [referring to the Adult Attachment Interview (AAI)]. [FN4B]
Dr. Cloitre found “that pure PTSD symptoms are a function of specific traumatic incidents, but the other symptoms she identified – affect dysregulation, mood regulation, anger expression, chronic suicidality, self-injury, disturbance in relations with self and others… do not occur in PTSD. They are rather a function of a disturbed attachment relationship,” van der Kolk repeated.
Yet psychiatry, he says, “is not good at treating attachment difficulties. There is very little treatment” of it. Innovative somatosensory healing programs at van der Kolk’s Trauma Center in Boston using “theater programs, yoga, martial arts for kids, etc. — to get them inter-personally attuned — are not standard treatment even though we do statistical research and publish it,” he notes.
The Body Keeps the Score
Because DTD happens before we have a thinking brain, the body is forced to store all the memories as somatic trauma. “There is somatization. The body keeps the score,” he says, the title of his latest book, “this is a somatic experience, and you become a terrified organism. Your immune system changes, your stress hormone system changes and your perception of your body changes.”
PTSD’s existence was hard to get recognized at first, too. It took Dr. van der Kolk and friends a chunk of the 1970s and ’80s to get the government to stop insisting that war trauma didn’t exist. Doctors finally established the diagnosis PTSD by showing that Vietnam vets were re-living discrete terrifying incidents from the past.
But “in fact there was no basis for any opinion about the prevalence” of any childhood trauma, even of childhood sexual abuse, before the 1995-1998 Adverse Childhood Experiences (ACE) Study, study co-director Dr. Vincent J. Felitti, MD, notes. “That’s because such information is almost completely protected by shame and secrecy, by families, and by individuals. Doctors also have been inhibited by our own ignorance and major gaps in our training, from asking into certain areas of patient history.” [ FN5]
In 1995 Felitti ran an obesity program at Kaiser Permanente in San Diego. But he had a 50% drop-out rate, just when those quitting were losing up to 100 pounds. “As we interviewed almost 300 of the dropouts, every other person spoke of having childhood sexual abuse; most of them seemed to have been waiting to tell someone after hiding it for years,” Felitti said. “They also often mentioned verbal and physical abuse and other traumatic experiences such as watching their mother being beaten.
“We wanted to know: to what degree does this happen in the whole population? That’s how we created the ACE Study. We took at first 8 and later a total of 10 categories of traumatic childhood experiences which we’d heard about from our obese patients, then found 17,421 average, middle-class adults who agreed to interviews.
“We were astonished to find that the percent of the general public who suffer from traumatic experiences in childhood and adolescence is far higher than imagined… Two-thirds (64-67%) of middle class subjects had one or more types of childhood trauma, and 38-42% had two or more types. One in six had an ACE Score of 4 or more; one in nine had an ACE Score of 5 or more.” In less privileged populations the numbers are far higher.
Similarly, Dr. van der Kolk describes a patient in the 1980s who could not recall if she were sexually abused, yet drew portraits of her family with menacing genitals. “So we went to the textbook — Freedman, Kaplan, & Sadock’s ‘Comprehensive Textbook of Psychiatry’ — with which I sat for my board exam in psychiatry. It said: ‘Incest is very rare; it happens in 1 out of 1.1 million women.’ At the time there were about 200 million Americans, so I thought, ‘Hmm… About 100 million women, 110 women are incest victims; how come 47 of them are in my office?’/” [FN4 Yale video.]
“The text says it is also very benign,” he went on quoting it: ‘There’s no agreement about the role of father-daughter incest as a source of psychopathology. The act offers an opportunity to test a fantasy whose consequences are found to be gratifying and pleasurable…In many cases it allows for a better adjustment to the external world. The large majority of them are none the worse for the experience ’. ” [FN7]
Developmental Trauma: Psychiatrists Still in Denial
But even today, until DTD is in the APA’s official Diagnostic and Statistical Manual of Mental Disorders (DSM), most mental health professionals will not diagnose or treat it, and no insurance company will cover it.
So in 2012 Dr. van der Kolk’s NCTSN network submitted data on 200,000 children around the world to the APA to document DTD. He spoke on DTD before the National Association of State Mental Health Directors, which treats 6.1 million patients a year with a $29 billion budget, and they wrote to the APA urging that DTD be included in the next DSM-5 in 2013.
But the APA refused and in June 2013, issued DSM-5 without mention of developmental trauma. Van der Kolk in his Yale video ridicules the APA for asking only two questions on child trauma in preparing DSM-5: “1. Can we assume life was pretty good growing up? and 2. Was anyone in your family a drug addict or an alcoholic?”
“Clearly our field would like to ignore social realities,” van der Kolk responds, “and study genes or biological functions — because for us to actually find out how the environment shapes the brain, would get us into very difficult situations.”
The APA refusal letter actually made a veiled dig against the Adverse Childhood Experience (ACE) Study and denied that “childhood adverse experiences” are a “substantive” problem – which is outrageous. Dr. van der Kolk read that letter at Yale in May 2013 and let ’em have it:
APA: “The consensus was there was just too little evidence to include DTD in the DSM-5. There have not been any published accounts about children with this disorder.”
Dr. vdK aside: “No, because it’s not in the textbooks!”
APA: “The notion that childhood adverse experiences lead to substantive developmental reduction is more clinical intuition than a research-based fact. “
Dr. vdK aside: “We submitted research data on 200,000 children from around the world to substantiate our diagnosis.”
APA: “The statements made cannot be backed up by prospective studies.”
Dr. vdK aside: “Actually, they can.”
Dr. van der Kolk could make a lot more money as a TV comedy star, after dealing with this idiocy for a lifetime. Despite the tragedy, his psychiatrist audience also had a good laugh — the APA is that absurd.
Developmental trauma is the “invisible” part of “the Silent Epidemic of Attachment Disorder.” [FN8]. DTD can happen as a by-product when a mother or her child are beaten or sexually abused – but it also happens on a wide-spread basis with no visible incident.
Perhaps 20-40% of our population goes through life never knowing they even have DTD. That’s why many of them go on to become leaders of industry and government. That’s why Dr. van der Kolk has said that the US Congress is “dissociated,” or they’d feel the simple human compassion to know that sending youth to war brings back a flood of PTSD suicides. (To me that means more than 50% of Congress has attachment problems, which is why they made a career of trying to control others. ) [FN9]
Commentsare encouraged, with the usual exceptions; rants, political speeches, off-color language, etc. are unlikely to post. Current software limits comments to 1030 characters (2 long paragraphs).
News blogs expand on my book Don’t Try This Alone: The Silent Epidemic of Attachment Disorder. Watch as my journey of recovery teaches me the hard way about Adult Attachment Disorder, Developmental Trauma, Attachment Theory, and the Adult Attachment Interview (AAI).
Medical Disclaimer:This website is for general information purposes only. It is simply my own research. Individuals should always see their health care provider or licensed psychotherapist before doing anything which they believe to be suggested or indicated herein. Any application of the material on this website is at the reader’s discretion and is the reader’s sole responsibility.
Footnotes
FN1 van der Kolk, Bessel, MD, “Developmental Trauma Disorder: Toward a rational diagnosis for children with complex trauma histories,” Psychiatric Annals 35:5, 401-408, May 2005 www.traumacenter.org/products/pdf_files/preprint_dev_trauma_disorder.pdf
This article also details how developmental trauma is attachment-based: “Early patterns of attachment inform the quality of information processing throughout life [11]. Secure infants learn to trust both what they feel and how theyunderstand the world…. (more),” he reports.
But “When caregivers are emotionally absent, inconsistent, frustrating, violent, intrusive, or neglectful, children are liable to become intolerably distressed and unlikely to develop a sense that the external environment is able to provide relief. Thus, children with insecure attachment patterns have trouble relying on others to help them, while unable to regulate their emotional states by themselves. As a result, they experience excessive anxiety, anger and longings to be taken care of. These feelings may become so extreme as to precipitate dissociative states or self-defeating aggression…”
Dr. van der Kolk has been Medical Director of The Trauma Center in Boston for 30 years (www.traumacenter.org).
FN2 Daniel Siegel, MD, et.al, “Trauma, Brain & Relationship: Helping Children Heal,” www.youtube.com/watch?v=jYyEEMlMMb0
Introductory video on Attachment Disorder and how development of the mind-body system can cause trauma. Copies at www.postinstitute.com/dvds.
FN3 Schore, Allan N., PhD, “Effects of Early Relational Trauma on Right Brain Development, Affect Regulation, & Infant Mental Health,” 2001, www.trauma-pages.com/a/schore-2001b.php
FN4B Cloitre, Marylene, et. al, (NYU Child Study Center, Department of Psychiatry, New York University Medical College, marylene.cloitre@nyumc.org), “Attachment organization, emotion regulation, and expectations of support in a clinical sample of women with childhood abuse histories,” Journal of Traumatic Stress, 2008 Jun;21(3):282-9. doi: 10.1002/jts.20339. Abstract: Despite the consistent documentation of an association between compromised attachment and clinical disorders, there are few empirical studies exploring factors that may mediate this relationship. This study evaluated the potential roles of emotion regulation and social support expectations in linking adult attachment classification and psychiatric impairment in 109 women with a history of childhood abuse and a variety of diagnosed psychiatric disorders. Path analysis confirmed that insecure attachment was associated with psychiatric impairment through the pathways of poor emotion regulation capacities and diminished expectations of support. Results suggest the relevance of attachment theory in understanding the myriad psychiatric outcomes associated with childhood maltreatment and in particular, the focal roles that emotion regulation and interpersonal expectations may play. http://www.ncbi.nlm.nih.gov/pubmed/18553408
FN5 Vincent J. Felitti, MD; Robert F. Anda, MD, MS; “The Lifelong Effects of Adverse Childhood Experiences,” Chapter 10 of Chadwick’s “Child Maltreatment,” Sexual Abuse and Psychological Maltreatment, Encyclopedic Vol 2 of 3, STM Learning, Inc., Saint Louis, p.203-215; March, 2014
FN6 Stevens, Jane, “The Adverse Childhood Experience Study” — the largest, most important public health study you never heard of — began in an obesity clinic,” ACEsTooHigh.com
FN7 Freedman, Alfred M., Kaplan, Harold I., & Sadock, Benjamin J., “Comprehensive Textbook of Psychiatry,” 2nd Edition, Williams and Wilkins Co., Baltimore, 1975; 2609 pages. Now in 9th edition; known since 4th edition as “Kaplan and Sadock’s.”
FN8 Lanius, Ruth A., MD; Vermetten, Eric; Pain, Claire; Editors, “The Impact of Early Life Trauma on Health and Disease: The Hidden Epidemic,” Cambridge University Press, 2010. “Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician,” American Academy of Pediatrics, 2012 (New York Times 1-7-12), and many more.
FN9 van der Kolk, Bessel, MD, “What Neuroscience Teaches Us About the Treatment of Trauma,” June 6, 2012 webcast, National Institute for the Clinical Application of Behavioral Medicine (NICABM) : Most of Congress is “dissociated,” van der Kolk told this 2012 globally-televised webcast, or they’d feel the simple human compassion to know that sending youth to war brings back a flood of PTSD suicides. We already knew from Korea and Vietnam that “for every solider that will die on the battlefield, there will be 30 suicides, as is happening right now,” van der Kolk said. But “society dissociates from the reality of it and then Congress says, ‘Oh, gosh, isn’t that amazing!’ No it’s not amazing, that’s what happens!”
Short promo clip: http://www.nicabm.com/nicabmblog/how-trauma-traps-survivors-in-the-past/
Link to buy video, mp3 audio, transcripts: http://www.nicabm.com/trauma-2012-new/
On Congress, see also http://www.theatlantic.com/politics/archive/2014/06/why-it-matters-that-politicians-have-no-experience-of-poverty/371857/
(Updated 4-12-17) Only 55% of us had “secure attachment” as infants, according to research on 6,282 infant-parent pairs during 1977-1999. This would worry us all if we knew what it meant, because the other 45% suffer “insecure attachment.” That means almost half of us have trouble with committed relationships. [1, 2]
This is because the attachment we had as kids continues all our lives, according to related research on over 10,500 adults during 1982-2009. Plus, we pass on our “insecurity” to our children. [3]
These are the “quiet blockbuster” results of two extended, linked studies. First, using the “Strange Situation” procedure, Dr. Mary Ainsworth and her successor Dr. Mary Main studied infant attachment. (Dr. Main & Dr. Daniel J. Siegel, above.)
Second, Dr. Main used the Adult Attachment Interview (AAI) to study the infant’s adult parents. Results showed that almost half the adults were not securely attached, either, and this corresponded to their own infants’ attachment.
This 45% “insecure” figure starts to explain why we’ve got a 50% divorce rate. If (like me) you’ve tried dating after divorce, it won’t surprise you that science shows almost half the adults out there can’t manage a secure, committed, relationship. Ouch, you’ve experienced it.
And if 45% of us were “insecurely attached” in 1999, what’s the rate in 2017? In the almost 20 years since, we’ve become an “e-society” with email, cell phones, texting and computers further trashing our ability to relate in person. Psychotherapists interviewed for this blog said that a round number of “about 50%” insecure attachment is conservative. Some say our insecure rate is higher.
In fact, the 2009 study of over 10,500 Adult Attachment Interviews said that secure attachment had fallen by another 17.1%, since the 1999 secure estimate of 55% above. That would mean 46% were secure in 2009 and the insecure rate was up to 54%–more than half the population. [3]
Here’s more “about 50%” data. The Adverse Childhood Experiences (ACE) Study showed that 66% of 17,337 middle class adults had one or more types of childhood trauma, and 42% had two or more types. In less privileged populations these numbers are over 70%. A U.S. average of all economic groups would show 50% or more suffer two or more types of ACE trauma.
That means, for example, they experienced both childhood physical and sexual abuse, or both childhood emotional abuse and neglect.
The ACE Study lists 10 such abuses, including traumas that happen to newborns (physical and emotional neglect). Such trauma puts children into “fight-flight,” a chronic state proven to shut down the organism’s capacity for feelings of attachment and love. [4]
Half of us have some degree of attachment trauma and don’t even know it. Let’s get informed; then we can heal. If we didn’t get securely attached as kids, we can develop “earned secure attachment.” “It’s possible to change attachment patterns,” as Dr. Main’s colleagues say. [5]
Strange Situation Experiment
Attachment Theory isn’t new; it just gets too little air time. British psychiatrist John Bowlby (left) developed it in the 1950s while working on the post-war orphan crisis. [6] Bowlby believed that all infants would seek to stay close to parents, since such “attachment” promotes survival. In 1952, he published a study of toddlers’ responses to separation from parents. It showed that “when toddlers were placed in unfamiliar surroundings that provided no stable caregivers, they underwent three… stages of response to separation: protest, despair, and finally detachment,” writes Dr. Main. [7]
Dr. Mary Ainsworth studied with Bowlby in London 1950-54, then researched his concept of “proximity-seeking behavior” in infant-mother pairs in Kampala, Uganda, published as “Infancy in Uganda” (1967). Then she found “astonishing similarities” in Baltimore, MD pairs. [7]
Ainsworth created the Strange Situation in the early 1970s, as a science experiment at Johns Hopkins in Baltimore to document this infant behavior. “Ainsworth structured the Strange Situation to include three of Bowlby’s ‘natural clues to danger’… to arouse babies to seek proximity” to the parent, Main says. Researchers watch and video-tape through one-way glass, as infant-mother pairs react to apparent danger. First a baby responds to a strange lab room; then to two entrances of a strange person; then to two different separations from its mother (details in footnote 8). [8]
Babies were expected to stay close to parents as Bowlby thought. Babies “that Ainsworth termed ‘secure,’ play and explore happily prior to separation; show signs of missing the parent during separation, such as crying and calling; seek proximity immediately upon the parent’s return; then return to play and exploration, ‘secure’ once again in the parent’s presence,” reports Main. [8]
But 30% of babies did notact secure–they avoided mom. They showed no preference between mom and the stranger. “While a majority of infants behaved as expected and were termed secure, to Ainsworth’s amazement six showed little or no distress at being left alone in the unfamiliar environment, then avoided and ignored the mother on her return,” Main reports (emphasis added). [7]
Ainsworth decided to categorize these babies separately as “avoidant” of mother. Now she had two types: (A) Insecure Avoidant and (B) Secure. She concluded that moms of avoidant babies didn’t respond or have the sensitivity to understand the babies’ real need, so infants felt “insecure.” [8]
Still later Ainsworth saw that of the insecure babies, some had yet a third reaction: actually, they were “ambivalent” about mom. They were very distressed when mom left, but on her return, they alternated between avoiding and frantic clinging–plus, they never calmed down. Research showed that ambivalent attachment results from moms who are sometimes available, sometimes not, so babies learn they can’t depend on people.
So “surprisingly, Ainsworth found that infant responses to separation and reunion fell into three distinct, coherently organized patterns of attachment,” and added a third category: (C) Insecure Ambivalent, Main reports. [8, 9]
By 1977 Ainsworth had developed an “American standard distribution” for infants of “about” (A) Insecure Avoidant 20%, (B) Secure 70%; and (C) Insecure Ambivalent 10%. By 1988, Strange Situation research using Ainsworth’s three categories had been done with 2,000 infant-parent pairs in 32 studies in 8 countries. Some countries varied, but global results averaged the same. [9]
Scary Parents
In 1973 Mary Main became Ainsworth’s grad student at Johns Hopkins in Baltimore, working on the Strange Situation experiments from their start. After her doctorate Main moved to Berkeley, to see if Ainsworth’s Kampala and Baltimore findings would replicate. [8] In 1977 Main did a Strange Situation study of 189 Bay Area infant-parent pairs which did replicate Ainsworth’s results. [8, 10]
But by 1979 Dr. Main was making her own discoveries—out of concern about the parents.
“In none of Ainsworth’s original observations was the possibility considered that some mothers… could also be frightening,” Main notes.
“For my dissertation at Johns Hopkins, I watched 50 children in the Strange Situation… Using Ainsworth’s three-part classification (secure, avoidant and ambivalent), I found at least five infants could not be classified…
“I had visited most of the mothers in their homes,” Main wrote, “and I knew that at least three of the five mothers of the un-classifiable infants had behaved most peculiarly with their offspring. One—frighteningly, to me—had treated her toddler as an animal.” [8]
Ainsworth was concerned, too; in fact, she’d put some babies in her Secure set only because they didn’t fit her other two sets, Main writes. [8]
By 1985, Main decided to “extend attachment theory to include the import of infant exposure to anomalous fear-arousing parental behaviors (Main & Hesse, 1990)… in conjunction with the discovery of a fourth Strange Situation attachment category, ‘insecure-disorganized/disoriented’ (or ‘D’) (Main & Solomon, 1990)…
“We proposed that fear of the parent could account for many instances of disorganized behavior, since the infant’s natural haven of safety will have simultaneously and paradoxically become the source of its alarm (Hesse & Main, 1999, 2000),” Main reports. [8 p.257; 11]
Main and Ainsworth agreed that some 15% of babies actually form a new, fourth group: (D) Insecure Disorganized. Their mothers were so frightening that the babies couldn’t develop any consistent response. These infants “exhibited a diverse array of inexplicable or overtly conflicted behaviors in the parent’s presence” including “disorganization, disorientation, and confusion,” Main wrote. This included crying loudly then suddenly freezing; ignoring the parent to rock on hands and knees; moving away; raising hand to mouth in fear; or swiping at the parent’s face. [8, 11]
This finding that 15% of average U.S. babies are so insecure they’re almost incoherent was so shocking, it was checked for years. [2, 10, 11] But the number held. Worse, among children of American adolescent mothers the rate is over 31%, and is over 25% in many Third World nations. [12]
To remove the 15% of disorganized babies from Ainsworth’s original estimate of 70% secure, would reduce the secure set to 55%. If so, Main would have four categories: avoidant 20%, secure 55%, ambivalent 10%, and disorganized, 15%. [1, 11]
What was up with parents that 45% of their kids couldn’t manage secure attachment?
That was how researchers read Main’s documents for the 20 years from 1990 to 2010. [ 2, 10, 11]
That 55% Figure
I first heard this “55% secure” figure in 2010 from therapist Dr. Henry Cloud, New York Times best-selling author of “Boundaries.” He’s also the author of “Safe People,” a book whose point is that many folks we meet are able to relate, but almost as many are not. Asked for numerical odds at a lecture, he said that 55% are securely attached but 45% are insecure. Later I asked therapists at a UCLA therapists’ conference, who also said that professionals commonly speak of 55% secure.
Checking online, I found an authoritative report in “Pediatric Child Health” by Dr. Diane Benoit, MD. “Infants with secure attachment greet and/or approach the caregiver and… are able to return to play, which occurs in 55% of the general population,” she writes.
“Infants with insecure-avoidant attachment fail to greet and/or approach, appear oblivious to their caregiver’s return… in 23% of the general population. Infants with insecure-resistant [ambivalent] attachment are extremely distressed by separations and cannot be soothed at reunions, displaying much distress and angry resistance” and can’t return to play, “in 8%.” Benoit earlier reports that “in normal, middle class families, about 15% of infants develop disorganized attachment.” Her first three categories above add to 86%, leaving 14% disorganized.
“Of the four patterns of attachment, secure, avoidant, resistant and disorganized, disorganized attachment in infancy and early childhood is recognized as a powerful predictor for serious psychopathology and maladjustment in children. Children with disorganized attachment are more vulnerable to stress, have problems with regulation and control of negative emotions, display oppositional, hostile, aggressive behaviours…” Dr. Benoit says (emphasis added). [1]
Similar numbers were reported by van IJzendoorn, one of Benoit’s sources, in 1999. His global total of 6,282 infants in 10 countries was 51.5% secure, 17.4% avoidant, 10.6% ambivalent, and 20.5% disorganized. (Data from developing nations perhaps produced the large disorganized rate.) Statistics for 2,104 North American infants were cited as 62% secure, 15% avoidant, 9% ambivalent, and 15% disorganized. [2, p.233, p. 229]
“Studies show that between 35% and 45% of all children in the US experience some kind of attachment issue,” reported GoodTherapy.org, a respected therapists’ website [13]
“About 55 percent to 65 percent of children fall into the ‘secure’ attachment category,” wrote attachment scholar Sean Brotherson in 2005, “while about 10 percent to 15 percent show an ‘insecure-resistant/ambivalent’ pattern, 20 percent to 25 percent show an “insecure-avoidant” pattern and 15 percent to 20 percent an “insecure-disorganized.” [14]
“Disorganized” or Not?
Recently, however, there has been enough misuse of the term “disorganized” by courts and social services, that Dr. Main’s network seems to have resumed citing only the three 1978 Ainsworth categories.
“Main, Hesse, and Hesse (2011, p.441) have criticized the ‘widespread’ and ‘dangerous’ presumption that infants can be divided into four categories,” wrote History of Psychology magazine recently. “ ‘The reification of our work from its context… has lead readers to treat D as a category equivalent in kind to ABC, rather than recognizing it… runs orthogonal to the basic Ainsworth patterns’,” Dr. Judith Solomon is quoted to say. [15]
That would put securely-attached back up to Ainsworth’s 1978 figure of 70% – despite many studies showing our attachment rate has fallen. [3]
Yet in numerous writings over 20 years, Main, Solomon and colleagues called the disorganized group a “new fourth category.” They also repeatedly wrote that when only three categories were in use, most disorganized infants had been “forced” into the “secure” category. This happened only because they didn’t fit the other two categories, but in fact these infants were not secure, they often wrote.
That’s why the use of four categories is so “widespread,” as in the quote from Dr. Benoit above about the “four patterns of attachment, secure, avoidant, resistant and disorganized.”
Perhaps others have abused the term “disorganized” to mis-label children as “hostile, aggressive, coercive” or to otherwise harm kids. Perhaps law suits have resulted from this. That’s awful.
Yet while I respect and revere Dr. Main’s group, the notion that 70% of flesh and blood Americans have suddenly become “secure” just by using different words, or due to lawsuits, makes no sense. It’s certainly not my experience nor the experience of any therapist with whom I’ve spoken.
It also leaves most of the 50% of us with emotional pain from attachment trauma alone, without recognition or a voice, and with no idea that we even need help, let alone any idea how to get healing. That’s why I’m speaking up.
Examples of the original wording by Dr. Main’s group feature:
“By 1985, our laboratory had developed a number of new methods for assessing attachment. Besides Ainsworth’s original tripartite analysis of the Strange Situation procedure… we emphasize… disorganized attachment, devised by us as a new category of infant Strange Situation behavior…” [8, p.257]
“The next discovery… was based on the simultaneous breakthrough reported by Main and Solomon (1986, 1990) that a fourth Strange Situatio classification—disorganized/disoriented—could now be recognized. Infants were placed in this fourth category (see Lyons-Ruth & Jacobvitz, Chapter 28, and Solomon & George, Chapter 18, this volume) when they failed to maintain the behavioral organization characteristic of those classified as secure, avoidant, or ambivalent/ resistant… by 1990 infants were termed disorganized/ disoriented in the Strange Situation when, for example, they approached the parent with head averted, put hand to mouth in a gesture indicative of apprehension…or rose to approach the parent, then fell prone to the floor…” [10, p.572]
“[T]he limits of the traditional Ainsworth et al. (1978) coding system became apparent because many children with an established background of abuse or neglect nevertheless had to be forced into the secure category… Disorganization of attachment is usually considered a type of insecure attachment…” 2, p.226]
“Our chapter begins with a review of previous studies reporting difficulties in “forcing” each infant in a given sample into one of the three major categories… However, the majority of these…disorganized-disoriented infants would have been identified as secure… had we forced them into the standard classification system.” [11, p.97-8]
Dr. Ainsworth herself, co-authoring a volume with Dr. Main in 1990, writes: “… it is acceptable to consider adding…the fourth D category that Main identified as disorganized… Now that so much careful work has been done to explore the ramifications of this new category, it may be accepted as a valuable extension of the Strange Situation classificatory system.” [16]
Whatever one thinks about categories, Dr. Benoit’s closing advise on achieving secure attachment says it all:
“During the first six months of life, promptly picking up a baby who is crying is associated with four major outcomes by the end of the first year of life. First, the baby cries less. Second, the baby has learned to self-soothe. Third, if the baby needs the caregiver to soothe him/her, the baby will respond more promptly. And finally, the caregiver who responded promptly and warmly most of the time (not all the time; nobody can respond ideally all of the time) to the baby’s cries, will have created secure, organized attachment with all of the associated benefits.” [1]
The Adult Attachment Interview (AAI)
Moving on to adults, by 1982 Main had seen enough disorganized babies to conclude that there must be a lot of scary parents.
Now she needed a way to document the behavior of the parents. [17] (Right: Dr. Main (center) receives the 2009 Bowlby-Ainsworth Attachment Award.)
That’s how the AAI came about. It was created in 1982 to discern the level of secure, loving attachment the parents had during their own childhoods with their babies’ grandparents. Parents were asked “both to described their attachment-related childhood experiences – especially their early relations with parents – and to evaluate the influence of these experiences on their development and current functioning.”
Parents were studied not just on facts they gave, but on how coherent a narrative they could produce quickly. That’s easy for folks who had a secure childhood, but difficult for folks who did not. The AAI questions are designed to “surprise the unconscious” to yield information about the “state of mind with regard to attachment” that might not otherwise show up. Each AAI was taped and transcribed verbatim. Then transcripts were classified by specific patterns by independent trained specialists. [18, 10]
In 1982 Main also created the “Berkeley Longitudinal Study” to take 67 Bay Area infant-parent pairs from her 1977 Strange Situation and study them for a generation. In 1977 the babies were 12-18 months old. Main and her team re-studied these pairs when the kids reached age 6 in 1982, and studied the kids again when they reached 19 in 1995. [8, 10] In 1982 Main and her team gave three different tests to the Bay Area pairs:
— 1. The parents were given the AAI (without their children). [8, 10]
— 2. The six year olds were again studied with their parents in the Strange Situation (as they’d been studied in 1977 as infants).
— 2. The “sixes” were also individually (without parents) given a new Separation Anxiety Test (SAT): they were shown pictures of children being separated from their parents, then asked how they felt. This was taped, transcribed and sorted by Main’s student Nancy Kaplan into Ainsworth’s three sets: secure, avoidant and ambivalent. [19, 8]
Dr Main’s initial 1982 AAI results were so important that it’s a tragedy that your doctor never learned this in medical school; your therapist (and mine) never heard of it; you’ve never heard of it; and so you have to read about it here, since the media doesn’t report it.
Amazing Results You’ve Never Heard
First: Main noticed that the initial 1982 adult AAIs fell into categories very similar to those into which infants had fallen years earlier in the Strange Situation. As Main had only Ainsworth’s three infant categories in 1982, she at first classified adults into Secure (matching infant “Secure”); Dismissing (matching infant “Avoidant”); and Preoccupied (matching infant “Ambivalent”). (Dr. Main and Dr. Hesse, above.)
Main was astonished to find that the more adults who took the AAI, the more the adult data (in three categories) statistically converged on Ainsworth’s “standard distribution” for infants: 20%, 70%, 10%. [10, p.552]
Second: the levels of adult attachment in the adults’ 1982 AAIs corresponded specifically to the attachment to that adult which their own infant exhibited in the 1977 Strange Situation. “Secure-autonomous (“valuing of attachment relationships and experiences) was associated with infant Strange Situation security,” reports Dr. Main’s co-author Dr. Erik Hesse, and this was true of all categories.
“Thus, a marked relation between a parent’s hour-long discussion of his or her own attachment history, and the offspring’s Strange Situation behavior 5 years previously, had been uncovered.” [10, p.552]
Third: the match of each parent’s own attachment with their baby’s attachment five years back was at an unheard-of level. It correlated 75% of the time, in a field where a 20% correlation is highly significant. [8, 10]
Fourth: the six year olds’ responses to parents in the Strange Situation in 1982 correlated strongly to their 1977 responses as infants — five years earlier. These kids at six responded to parents just as they had as infants, in the same percents. [7]
Fifth: the six year olds’ 1982 solo responses to the Separation Anxiety Test also produced the same results and percentages as their response to parents in the 1982 Strange Situation.
Sixth: In 1986, Main published her discovery of the fourth infant category of disorganized, and quickly found that if adults were sorted into four analogous categories, again results were the same.
“The next discovery regarding the AAI was based on the simultaneous breakthrough reported by Main and Solomon (1986, 1990) that a fourth Strange Situation (infant) classification—disorganized/disoriented—could now be recognized,” Hesse reports. “By 1990, it had been shown that unresolved AAI status in a parent was predictive of disorganized attachment in the infant… 91% of unresolved mothers had infants who had been judged disorganized with them in the Strange Situation 5 years earlier…
“Thus there was now an AAI category corresponding to and predictive of each of the four Strange Situation categories… In 1996… in a combined (meta-anlytic) sample of 584 non-clinical mothers… a four-way analysis showed… 16% dismissing, 55% secure-autonomous, 9% preoccupied, and 19% unresolved,” (emphasis added). In 2008, a global sample of AAIs for 1,012 average mothers showed the same results. [10]
These numbers for adults are astonishingly similar to the statistics for infants cited by Benoit, van IJzendoorn and others reviewed above: 23% avoidant, 55% secure, 8% ambivalent, and 14% disorganized.
“Just over 50 percent are secure, around 20 percent are anxious, 25 percent are avoidant, and the remaining 3 to 5 percent fall into a fourth, less common disorganized category,” Dr. Amir Levine, MD states in the popular 2010 book “Attached,” speaking of adults. [20]
Finally: When the 1977 infants reached age 19 in 1995, they too were given the Adult Attachment Interview. Again results correlated strongly: the 19 year olds’ responses in the 1995 AAI correlated precisely to their infant behavior in the 1977 Strange Situation, their 1982 behavior at six, and to their parents’ 1982 responses to the AAI. [8]
Bottom line? The Strange Situation predicts an infant’s emotional behavior for life, and the AAI proves it. [8, 10]
“Researchers worldwide have replicated the relation originally uncovered in the Bay Area study between a parent’s status in the Adult Attachment Interview and an infant’s Strange Situation response to that same parent… The same average parent-to-child, secure/insecure match of 75% holds even when the interview is conducted before birth of the first child…
“Describing the strength of this relation across studies conducted several years ago, van IJzendoorn (1995) calculated that it would take 1,087 further attempted replications, every one yielding insignificant results, to reduce the present relation between adult and infant attachment status to insignificance,” Main concluded in 2000 (emphasis added). [7, p.1091]
That’s not all.
Our attachment rate has fallen even further since 1999-2000, around the time that electronic devices began to increasingly replace human interaction.
“Well-developed human beings can self-regulate their emotional state by being with other humans. But what about people who regulate their emotional state with objects?” i.e. electronics, warned neuroscientist Dr. Stephen Porges in 2014.
“We’re in a world now being literally pushed on us, by people who are challenged in their own social and emotional regulation, and we’re calling this ‘social networking.’ We’re using computers, we’re texting — we’re stripping the human interaction from all interactions… We’re allowing the world to be organized upon the principles of individuals who have difficulty regulating emotionally in the presence of other human beings.” [21]
Harsh economic reality, meanwhile, has turned parents who can still manage to give attentive, attuned care to infants into an endangered species.
“For decades to protect the mother-infant bonding, there were families around it, there weren’t single individuals raising babies, there wasn’t early day care,” warned UCLA’s Dr. Allan Schore in a 2012 interview.
“The early day protections have been lost,” he said, “so as a result… there is an increase in psychiatric disorders in this country and the reason is that we have not protected this early phase of infant life, the early mother bonding…”
Schore, the top attachment scholar known as the “American Bowlby,” cited the 2009 study of 10,000 adult AAIs using three attachment categories which showed that from 1999 to 2009, secure attachment fell by 17.1%. [3]
Using four attachment categories, if 55% were secure in 1999, then after a 17% drop, only 46% were secure in 2009.
That means 54% of the population was insecure as of 2009, if disorganized infants have not simply disappeared.
This insecure percentage has risen since 2009, and will continue to rise, as long as we raise infants in a society flooded with enough electronic devices and bad economic priorities to render their parents incapable of attachment.
A first step would be to address the information and policy vacuum regarding this “silent epidemic.” [22]
Commentsare encouraged, with the usual exceptions; rants, political speeches, off-color language, etc. are unlikely to post. Current software limits comments to 1030 characters (2 long paragraphs).
News blogs expand on my book Don’t Try This Alone: The Silent Epidemic of Attachment Disorder. Watch as my journey of recovery teaches me the hard way about Adult Attachment Disorder, Developmental Trauma, Attachment Theory, and the Adult Attachment Interview (AAI).
Medical Disclaimer:This website is for general information purposes only. It is simply my own research. Individuals should always see their health care provider or licensed psychotherapist before doing anything which they believe to be suggested or indicated herein. Any application of the material on this website is at the reader’s discretion and is the reader’s sole responsibility.
Footnotes
1 Benoit, Diane, MD, FRCPC (2004) “Infant-parent attachment: Definition, types, antecedents, measurement and outcome,” Paediatr Child Health, Oct 2004; 9(8) p. 541–545, retrieved April 12, 2017 from: www.ncbi.nlm.nih.gov/pmc/articles/PMC2724160/ “Infants with secure attachment greet and/or approach the caregiver and… are able to return to play, which occurs in 55% of the general population… Infants with insecure-avoidant attachment fail to greet and/or approach, appear oblivious to their caregiver’s return… in 23% of the general population. Infants with insecure-resistant [ambivalent] attachment are extremely distressed by separations and cannot be soothed at reunions, displaying much distress and angry resistance” and can’t return to play, “in 8%.” Benoit earlier reports that “in normal, middle class families, about 15% of infants develop disorganized attachment.” Her first three categories above add to 86%, leaving 14% disorganized.
2 van IJzendoorn MH, Schuengel C, Bakermans-Kranenburg MJ (1999) “Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants and sequelae.” Dev Psychopathol. 1999; 11:225–49. https://openaccess.leidenuniv.nl/bitstream/handle/1887/1530/168_212.pdf?sequence=1 “During the past 10 years nearly 80 studies on disorganized attachment involving more than 6,000 infant-parent dyads [6,281 pairs total, Table 1, p.233] have been carried out….In normal middle class families about 15% of the infants develop disorganized attachment behavior. In other social contexts and clinical groups this percent may become twice or even three times higher (eg in cases of maltreatment) … Disorganization… is usually considered a type of insecure attachment.”
3 Bakermans-Kranenburg MJ, van IJzendoorn MH (2009) “The first 10,000 Adult Attachment Interviews,” Attach Hum Dev. 2009 May; 11(3): 223-63. Retrieved April 12, 2017 from https://www.researchgate.net/
publication/24440045_The_first_10000_Adult_Attachment_Interviews_
Distributions_of_adult_attachment_representations_in_clinical_and
_non-clinical_groups http://www.ncbi.nlm.nih.gov/pubmed/19455453 This study showed a 17.1% drop in the secure category from the authors’ previous 1999 study to 2009. It used adult analogs of only Ainsworth’s three 1978 categories: 20% dismissing, 70% secure, 10% preoccupied (=100%). The 17.1% secure drop was reported as 23% dismissing, 58% secure, 19% preoccupied (=100%). It also showed “18% additionally coded for unresolved loss or other trauma.” Many of the 18% would be classed “disorganized” were all four categories used, but instead were “forced” into three categories. Since historically most disorganized subjects were “forced” into the secure category, the 58% secure number includes a significant number of disorganized. –Interview with Dr. Allan N. Schore by David Roy Green, World Healing Electronic Network, July 2012, minute 39, retrieved April 12, 2017 from http://whenworldwide.org/films/dr-allan-n-schore-full-interview/ Schore cites the secure attachment drop in the 2009 study above. “There is concern about this… that what was there for decades to protect the mother-infant bonding situation, there were families around it, there weren’t single individuals raising babies, there wasn’t early day care… the early day protections have been lost…so as a result of that, I’m now writing that there is an increase in psychiatric disorders in this country and the reasons is that we have not protected this early phase of infant life, the early mother bonding…”
4 Felitti VJ, MD; Anda RF,MD, et. al, 1998, “Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study,” American Journal of Preventive Medicine 1998;14:245–258. Detailed article: http://acestoohigh.com/2012/10/03/the-adverse-childhood-experiences-study-the-largest-most-important-public-health-study-you-never-heard-of-began-in-an-obesity-clinic/ For a popular text, see Karr-Morse, Robin, Wiley, Meredith, “Scared Sick,” Penguin Basic Books, 2012
5Siegel, Daniel J. , MD, “The Developing Mind: How Relationships and the Brain interact to shape who we are,” 1999 Guilford Press. Earned secure attachment occurs when we began life with insecure attachment, but “are now securely attached… individuals whose experiences of childhood… produce insecure attachment (avoidant, ambivalent, or disorganized),” but “…had a significant emotional relationship with a close friend, romantic partner, or therapist, which allowed them to develop… secure” attachment.
—Dr. Mary Main, Dr. Erik Hesse, Dr. Daniel J. Siegel, Dr. Marion Solomon, “Adult Attachment Interview with Mary Main,” Lifespan Learning Institute, Los Angeles, Jul 9, 2010 video: https://www.youtube.com/watch?v=YJTGbVc7EJY “It is possible to change attachment patterns, and we can help people as therapists to get the kind of new experiences that creates changes within people especially given the neuroplasticity of the brain,” says Dr. Solomon.
—Siegel, Daniel J. , MD, “The Mindful Therapist: A Clinician’s Guide to Mindsight and Neural Integration,” W.W. Norton, 2010; “Mindsight: The New Science of Personal Transformation,” Random House, 2010 “Mindfulness has been shown to be effective in healing insecure attachment. The purpose of both psychotherapy and mindfulness practice is to provide this internalized secure base. Attunement, whether it is internal in mindfulness, or interpersonal in attachment, is what leads to a sense of secure base.”
—Siegel, 2007, Wallin, 2007, p. 5-6 “The regular exercise of mindful awareness seems to promote the same benefits–bodily and affective self-regulation, attuned communication with others, insight, empathy, and the like–that research has found to be associated with childhood histories of secure attachment,” Siegel writes. “ Mindfulness and secure attachment alike are capable of generating… the same invaluable psychological resource: an internalized secure base.”
6 Bowlby, John, “The Nature of a Child’s Tie to His Mother,” British Psychoanalytical Society, London, 1958; “Attachment and Loss,” New York, Basic Books, 1969
7 Main, Mary, 2000, “The Adult Attachment Interview: Fear, attention, safety and discourse processes;” also titled “The Organized Categories of Infant, Child, and Adult Attachment: Flexible vs. Inflexible Attention Under Attachment-Related Stress,” Jour of Amer Psychoanalytic Assoc, 48:1055-1095; 2000. *p.1091: “The same average parent-to-child, secure/insecure match of 75% holds even when the interview is conducted before birth of the first child…” Retrieved March 14, 2014 from Lifespanlearn.org/documents/Main.pdf
8 Main, Mary, 2005, with Hesse, Erik & Kaplan, Nancy, “Predictability of Attachment Behavior and Representational Processes at 1, 6, and 19 Years of Age – The Berkeley Longitudinal Study,” Chapter 10 of “Attachment from Infancy to Adulthood: The Major Longitudinal Studies,” edited by Klaus E. Grossmann, Karin Grossmann, and Everett Waters, pp. 245–304, New York: Guilford Press. Main refers to it as “Regensburg;” retrieved June 4, 2014 from https://lifespanlearn.org/documents/5.Main Regensburg 2005 .pdf
–Main’s summary of the Strange Situation in this document:
“Ainsworth structured the Strange Situation procedure to include three of Bowlby’s ‘natural clues to danger’ in eight episodes: 1. Introduction to the room. 2. Mother and infant are left alone in a toy-filled environment whose unfamiliarity supplies the first natural clue to danger. However, the mother’s presence is expected to provide the infant with security sufficient for exploration and/or play. 3. Providing a second clue to danger, a stranger joins the mother and infant. 4. The mother leaves the infant with the stranger, providing two combined clues to increased danger. 5. The mother returns, and the stranger departs…. Many infants initially seek proximity but then, reassured of their mothers’ nearness, resume play. 6. The mother leaves, and the infant remains entirely alone in the unfamiliar setting. Infant distress can be strong at this point, and this episode is often terminated rapidly. 7. The stranger, rather than the mother, enters the room. 8. The mother returns… By now, most infants are expected to be crying, and actively not only seeking proximity to mothers, but also… indicating a strong desire to be held… Nonetheless, they are expected to settle and renew interest in exploration and play…
“Somewhat surprisingly, Ainsworth found that infant responses to separation and reunion in this procedure fell into three distinct, coherently organized patterns of attachment (“secure,” “insecure-avoidant,” and “insecure-ambivalent” (Ainsworth, Blehar, Waters, & Wall, 1978)… Given the length and complexity of this chapter, we suggest individuals divide reading to its three central parts (secure attachment, pp. 261–273; avoidant attachment, pp. 273–279; and disorganized attachment pp. 279–288).”
9 van Ijzendoorn, Marinus H.; Kroonenberg, Pieter M. (1988) “Cross-Cultural Patterns of Attachment: A Meta-Analysis of the Strange Situation,” Child Development,Vol 59 No 1, Feb 1988, p.147–56; (1988 global replication of Ainsworth’s three categories; written before Main’s 4th category developed 1986-1990). Retrieved July 2, 2016 from https://openaccess.leidenuniv.nl/bitstream/handle/1887/11634/7_702_111.pdf
—Ainsworth, Mary D.S., Blehar, M.C., et al, “Patterns of attachment: A psychological study of the Strange Situation,” Erlbaum, Hillsdale, NJ, 1978
10 Hesse, E., (2008) “The Adult Attachment Interview: Protocol, Method of Analysis, and Empirical Studies,” Chapter 25 of Cassidy, Jude & Shaver, Phillip R. (Eds), “Handbook of Attachment: Theory, research, and clinical applications,” 2nd edition, 2008, p. 552-598, New York, Guilford Press, retrieved June 4, 2014 from http://icpla.edu/wp-content/uploads/2012/10/Hesse-E.-Adult-Attachment-Int-Protocol-Method-ch.-25.pdf
—van IJzendoorn MH & Bakermans-Kranenburg,MJ (1996). “Attachment representations in mothers, fathers, adolescents and clinical groups,” Journal of Consulting and Clinical Psychology Vol 64(1), Feb 1996, 8-21. http://dx.doi.org/10.1037/0022-006X.64.1.8
11 Main, M., & Solomon, J. (1990). “Procedures for identifying infants as disorganized/disoriented during the Ainsworth strange situation,” in Greenberg, M. T., Cicchetti, D., & Cummings, M. (Eds.),. Attachment in the preschool years: Theory, research, and intervention (pp. 121-160), University of Chicago Press
—Main M, & Hesse E. (1990). “Parents’ unresolved traumatic experiences are related to infant disorganized attachment status: Is frightened and/or frightening behavior the linking mechanism?” Chapter 5 in: Greenberg MT, Cicchetti D, Cummings EM, eds., Attachment in the Preschool Years, University of Chicago Press; 1990 p 161–82
– Main M, & Solomon J (1986). “Discovery of an insecure disoriented attachment pattern: procedures, findings and implications for the classification of behavior,” in Brazelton T, Youngman M. Affective Development in Infancy. Norwood, NJ: Ablex; 1986. p. 95–124. https://www.scribd.com/document/253355881/Discovery-of-an-Insecure-Disorganized-Disoriented-Attachment-Pattern-Main-Solomon-1986
p.96 “In this chapter we describe commonalities observed in the behavior of 55 12- to 20-month-old [55 twelve- to twenty-month-old] infants whose strange situation behavior could not be classified using the traditional (A,B,C) classification system, infants who would nonetheless have been assigned (“forced”) into one of these three classifications.
p.97: Our chapter begins with a review of previous studies reporting difficulties in “forcing” each infant in a given sample into one of the three major categories.
p.98: “However, the majority of these “unclassified” (now, disorganized-disoriented) infants would have been identified as secure (group B) with the parent in the Strange Situation, had we forced them into the standard classification system.”
12 “Among children of American adolescent mothers, the rate is over 31% (Broussard 1995). Disorganized attachment is also common among the Dogon of Mali (~25%, True et al 2001), infants living on the outskirts of Cape Town, South Africa (~26%, Tomlinson et al 2005) and undernourished children in Chile (Waters and Valenzuela 1999),” reports [1] above.
13 “Attachment Issues,” unsigned, GoodTherapy.Org, July 3, 2015, retrieved April 3, 2017 from http://www.goodtherapy.org/learn-about-therapy/issues/attachment ]
14 “Understanding Attachment in Young Children,” Brotherson, Sean, Bright Beginnings #6, Oct. 2005, North Dakota State University, Fargo, ND, retrieved April 3, 2017 from http://www.ag.ndsu.edu/pubs/yf/famsci/fs617.pdf
15 “The Emergence of the Disorganized/Disoriented (D) Attachment Classification, 1979–1982,” by Robbie Duschinsky, Hist Psychol. 2015 Feb; 18(1): 32–46, retrieved 4-10-17 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4321742/ Cited within which: “Attachment theory and research: Overview with suggested applications to child custody,” Main M., Hesse E., & Hesse S., Family Court Review, 49, 426–463, 2011 ]
16 Ainsworth, Mary, PhD, “Epilogue: Some Considerations Regarding Theory and Assessment Relevent to Attachments beyond Infancy,” in “Attachment in the Preschool Years,” ed. M.T. Greenberg, D. Ciccheti & E.M. Cummings, Chicago University Press, 1990, p463-488; quote p.480.
17 George, Carol, Kaplan, Nancy, & Main, Mary, “Adult Attachment Interview,” Unpublished MS, Department of Psychology, University of California at Berkeley, third ed. 1996. Original 74-page MS dated 1984, 1985, 1996. Described in [10] Hesse 2008. Retrieved March 20, 2014 from http://stantatkin.com/wp-content/uploads/2012/04/AAI-Protocol.pdf, now removed. See also Main 1985; Main & Goldwyn 1984
18 Main, Mary B., “Adult Attachment Interview Protocol,” 11 pgs, 20 questions, no date or publisher. Dr. Main requires intensive training for use of the AAI. The questions per se, marked “Do not reproduce this material without permission of the author,” were retrieved most recently April 12, 2017 from http://www.psychology.sunysb.edu/attachment/measures/content/aai_interview.pdf
UCLA’s Lifespan Learning Institute in Los Angeles holds AAI workshops and has an extensive CD lectures on the AAI at www.lifespanlearn.org
19 Kaplan, Nancy, (1987), Separation Anxiety Test (SAT): “Individual differences in six-year-olds’ thoughts about separation: Predicted to actual experiences of separation,” Unpublished doctoral dissertation, University of California, Berkeley.
— Kaplan, N. (2003, April), “The development of attachment in the Bay Area study: One year, six years, nineteen years of age.” Paper at the biennial meeting of the Society for Research in Child Development, Tampa, FL.
20 “Attached: The New Science of Adult Attachment,” Dr. Amir Levine, MD & Rachel Heller, MA, Tarcher 2010; useful reviews at http://www.goodreads.com/book/show/9547888-attached
21 Porges, Stephen, PhD, p. 15 of “Polyvagal Theory,” National Institute for the Clinical Application of Behavioral Medicine (NICABM), April 2012, retrieved July 21, 2014 from http://www.stephenporges.com/images/NICABM%20April%202012.pdf
The Adverse Childhood Experiences (ACE) Study showed that for 17,337 patients, childhood trauma correlated to serious adult medical conditions. “Contrary to conventional belief," says co-Director Vincent Felitti, MD, "time does not heal all wounds, since humans convert traumatic emotional experiences in childhood into organic disease later in life.”
FEATURED BOOKS – QUOTES
"Too many Americans are spurred to achieve, rather than to attach." --A General Theory of Love
"Trying to fix the heart using the head, is like trying to paint with a hammer - it only makes a mess."
"You can be strong - or you can be human."
-- Grief Recovery Handbook
"Gosh, I shoulda checked the milligramage! Oh, well, Live and Learn." -- Working Girl
"Any book you haven't thrown across the room at least once because it smashed your world view, probably isn't worth a long shelf life." -- Kathy
"Mental health. For everything else there's MasterCard." -- Kathy
The Adverse Childhood Experiences (ACE) Study showed that for 17,337 patients, childhood trauma correlated to serious adult medical conditions. “Contrary to conventional belief," says co-Director Vincent Felitti, MD, "time does not heal all wounds, since humans convert traumatic emotional experiences in childhood into organic disease later in life.”
"Trying to fix the heart using the head, is like trying to paint with a hammer - it only makes a mess."
"You can be strong - or you can be human."
-- Grief Recovery Handbook
"Gosh, I shoulda checked the milligramage! Oh, well, Live and Learn." -- Working Girl
"Any book you haven't thrown across the room at least once because it smashed your world view, probably isn't worth a long shelf life." -- Kathy
"Mental health. For everything else there's MasterCard." -- Kathy
 “Bessel van der Kolk wants to change the way we heal a traumatized mind — by starting with the body,” reports Jeneen Interlandi in the New York Times Magazine May 22. (Dr. van der Kolk in session drawn by Matthew Woodson for the Times.)
“Bessel van der Kolk wants to change the way we heal a traumatized mind — by starting with the body,” reports Jeneen Interlandi in the New York Times Magazine May 22. (Dr. van der Kolk in session drawn by Matthew Woodson for the Times.)