What books and resources would you recommend for trauma?
I really recommend Dr. Allan Schore’s Sept 2014 Oslo speech video “The Most Important Years;” on my Resources tab, see the subtab on Audios & Videos. Dr. Schore (left) explains that babies are born screaming in pain because we’re designed for an adult’s emotional brain to show us “Someone cares, I can relax.” Mom’s love actually creates the neural networks in a baby’s brain needed to calm down, Schore wrote in the’ 90s. Now, in the last 5 years, brain scans have proven him correct. But with infant developmental trauma and attachment disorder, no adult showed us how to calm, so we never did. Infant emotions are still crying painfully deep inside us, says Schore. We’re unaware of it, but that is the cause of our anxiety, fear, anger, and misery.
Several healing tools are really helping me now. Links to all these below are on my Resources tab, sub-tab Healing Tools. I’m sorry to keep mentioning my website but I was forced to build it when I couldn’t find all this centralized anywhere else. My home page has almost 40,000 hits; my book tab over 12,000 hits and there are 4 more tabs. It gets hits because there’s a large amount of content on my pages. Here are the healing tools:
Neurofeedback is a computer program which therapists use to train clients to calm brain waves. We with early neglect and abuse have disorganized brains and fear circuits dominate. Neurofeedback can calm this by growing new neural networks, the way a mother grows a baby’s neural networks. I was moved to tears by Sebern Fisher’s recent interview “Neurofeedback in the Treatment of Developmental Trauma” on ShrinkRap radio, as she described how necessary love and attachment are to the creation of a human brain.
EMDR can resolve trauma using bilateral eye motion, bilateral sounds, or even tapping on either foot. When a therapist moves a finger from side to side before the patient’s eyes, it guides the eyes to move naturally as in rapid eye dreaming. That’s where we process most trauma. That means, we move traumatic memories out of short-term memory banks where it feels like a terrifying flash happening “right now,” into long-term memory banks where we feel it’s past, and we’re “over it.
Tapping: For years I’ve used tapping, aka Emotional Freedom Technique (EFT). We use fingertips to tap a few times on 9 of the body’s acupuncture points. It’s a fantastic aid in calming down, or even just getting to sleep at 2 am. I used it again just this morning to release a pile of anger.
Meditation: Meditation is where we ultimately need to go to fully heal, but it can be terrifying for us with infant trauma. To get started, we can work with our therapist on it, and meditate in groups. Please check Dr. Tara Brach’s “Basic Elements of Meditation Practice” videos on youtube; it’s also on my Resources tab, sub tab Audio & Video.
Books: on my Resources tab, look for the subtab on Books:
–“The Grief Recovery Handbook” by John James & Russell Friedman
–“A General Theory of Love”, Thomas Lewis, Richard Lannon et al; 2000.
–“Healing Trauma: A Pioneering Program for Restoring the Wisdom of Your Body,” Peter A Levine
–“Changes that Heal,” Dr. Henry Cloud
–“The Body Keeps the Score” Dr. Bessel van der Kolk, MD
Didn’t you say recently that there’s a lot of trauma in high places?
Yes, in part because emotional abuse is really hard to spot. Emotional abuse alone can be just as damaging as overt abuse, but I didn’t know I had trauma the whole time I was a high-functioning business gal with a math degree, working with rocket scientists. When I found out I had trauma, I used to say, “Nobody beat me or raped me. What’s wrongwith me!?”
What’s wrong was, I had a huge left thinking brain, but an infant’s right emotional brain that took a lot of damage. As Allan Schore says, when the mom doesn’t grow the infant’s right brain, the child’s left brain often over-develops in an effort to control the emotional chaos. My mom didn’t hold me as an infant or show me “it’s safe out here so you can stop crying,” to grow my right brain. So it remained an infant right brain. Instead, I learned that “it’s dangerous as heck out here, the world is scary.” I probably didn’t stop crying until my left brain grew myelin and began to think at 2 1/2 and I realized, cognitively, that if I didn’t shut up, they’d swat me.
I’ve been told: “Most people with what you have take it to the grave because they’re so intelligent, no one imagines anything’s wrong.” One thing motivating me to finish this book is: I’m betting that 20 to 40% of smart people in high places have infant or child trauma hiding inside where no one can tell, just as I did. Maybe my book can help them wake up.
That’s why our corporations, governments and so forth make a lot of un-compassionate decisions. No one showed them how to do compassion as kids. That’s why wee spend over $80 billion a year to drug school kids into being quiet, but there’s no funding for serious therapy for children.
Maybe my book will help people see reality. Allan Schore said in his Oslo video that UNICEF put out a report in 2013 saying society needs a massive shift of resources toward making sure at least the child, from conception to age 3 at least, and families with young children, get major public support to try to stop child trauma at the source. $80 billion would sure help.
Any closing thoughts? Sebern Fisher hit it on the nose: the real answer to trauma is love. Babies need our mothers to love us, to even just have the brain cells for emotional well-being. “We need to know that the Big Person who’s taking care of us, loves us,” says Dr. Henry Cloud, and then gradually a baby learns to grow “love inside” he says.
Or Not. What if I didn’t get love as an infant? Then emotional chunks of me are an infant’s emotions, and I need to find out about that. Then I need to go where I can get that part of me loved! Not to new parents, but I do need to feel the kind of love a good parent gives. And not to romance; we don’t want an infant or toddler on Match.com. Instead, I need to learn that I can receive platonic love from a really fine therapist, and that I can love them back. I need to learn that I can do deep platonic love with my Grief Partners and platonic friends at church or in small groups or yoga or meditation groups. I need to feel and give unconditional platonic love.
——————
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
————- Commentsare encouraged with the usual exceptions; rants, political speeches, off-color language, etc. are unlikely to post. Starting 8-22-16, software will limit comments to 1030 characters (2 long paragraphs) a while, until we get new software to take longer comments again.
The interview summarizes my work: my trauma history, what I’ve done to heal with good therapy, and my sorry adventures into what does not work, such as sub-par therapy. We noted the prevalence of child trauma, how it’s likely affecting a high percent of government and corporate leaders, and the need to educate and help them. Here are interview excerpts:
What is a quote that inspires you that is related to trauma? “Too many Americans are spurred to achieve, rather than to attach,” says A General Theory of Love; that’s at the core of our society’s illness. We’re rushed to compete and get the grade from age 5 or even Baby Einstein age, but there’s little talk of how to learn to attach compassionately to other human beings. But we are mammals, and we literally need attachment to other mammals, physiologically as well as emotionally, just to live. The book, which is by three psychiatrist MDs, demonstrates that unless we reverse this priority, our society can only get sicker.
Where are you from and what type of work are you doing? I’m from the New York City area, then lived 20 years in the Washington DC area. Now I live in Orange County, Southern California. I run a website with resources on attachment disorder, AttachmentDisorderHealing.com , and I’m writing a book about how I only discovered my severe attachment trauma after I hit age 50, and how I’m healing.
What is your story of trauma and recovery?
I was a high-performer who’d barely even heard of trauma. Suddenly I was divorced from a 27-year marriage, bankrupt, and homeless. “I married a bad man, now I’ll find a good man,” I thought. But I only found more abusive men, and it hit me: the common denominator is me! Something’s wrong with me. Then both my parents died in 2008, but when my Dad died, I couldn’t cry. “Wow, I’m really sick,” I said, and took myself to therapy. But I found 3 poor therapists who made me sicker, almost to the point of suicide. So in 2009 I quit therapy. What does not work is bad therapy.
Then I got something which does work, the Grief Recovery Handbook, which instructs us how to read letters to a Grief Partner about what’s hurting us emotionally. I wanted to heal from my marriage so I could date, so I read letters about my 27-year marriage to my partners for two years. But I didn’t feel better; I only found more pain. Reading about my marriage regressed me back to about when I met my ex at 18, but still more pain. Then I read letters about my Dad that regressed me back to age 5.
I removed 40 years of denial like rocks off my soul by releasing the anger and sorrow. But I didn’t have anything under the denial; the further back I went, I just found more pain. Then I read letters to my Mom that regressed me back to infancy. It’s all on AttachmentDisorderHealing on the New Book tab, in my Preface: “The Silent Epidemic.”
What have you done that helped with trauma and what did not work?
I discovered I was maybe 2 weeks old inside. It was so terrifying that this time I did a huge amount of research, found a really good attachment-based psychotherapist and went back to therapy in 2011. Thus my book title: “Don’t Try This at Home.” Don’t go it alone. What works is: 1. Do get a qualified attachment-based therapist but you must do serious research to find a good one. 2. The Grief Recovery Handbook works to get rid of denial, but with severe infant trauma, don’t do it unsupervised! That was my error. 3. Then what actually healed my trauma was Body Work; Dr. Peter A. Levine’s Somatic Experiencing method helped me enormously. For Body Work, go to AttachmentDisorderHealing; fifth tab from left Featured Topics. Subtab item #4 is Grief Handbook, then subtab item #5 is Healing: Body Work, with links to videos and books.
What advice would you give to those dealing with their own trauma?
I can only tell you what I learned: Don’t, don’t, don’t try this at home; I’ve put my last nickel into a good attachment-based psychotherapist. Second, later I discovered the Adult Attachment Interview (AAI) and I wish I’d had that at the outset, to find out scientifically how bad and what type my trauma is. On AttachmentDisorderHealing see the 4th tab Blogs for my blog on the AAI. Third, I worked the Grief Recovery Handbook (GRH) with a partner but I wish I’d kept a therapist thoroughly informed, it was dangerous not to. GRH can get rid of denial barriers so we can benefit from the next deeper steps. Fourth and most important is: Body Work.
Not reading books about Body Work – doing body work. Reading a book about singing is different from physically singing; reading a book about sex is, well, you know…. We need to do Body Work, not hide in books.
But remember: Body Work won’t get through to us unless we do the other steps first, especially if we have 20 or 40 years of denial to bust through.
Why can’t some Moms help their babies calm down?
Sadly, because Mom’s mom didn’t show her how, and grandma’s mom didn’t show her how; in my family I’ve traced it back to the 1800s and that happens a lot: inter-generational trauma. That’s why I’m not satisfied with programs for child trauma alone. We need those but we need more.
Fifty percent of parents out there themselves experienced some degree of childhood trauma, as the ACE Study shows. So it’s baked into their brain cells to pass it on and traumatize their children, mildly or wildly. Unless we have mass-based trauma healing programs for at least child-bearing aged adults, we can’t stop the cycle.
You can’t just hand a young couple a book and tell them carry the baby in front. If they’re deeply wounded, they don’t have the biological capacity to attune to another human being, and they need to learn that, which means serious psychological work. Otherwise they’re going to hurt babies and others until they get real emotional healing.
More excerpts next time…
——————
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
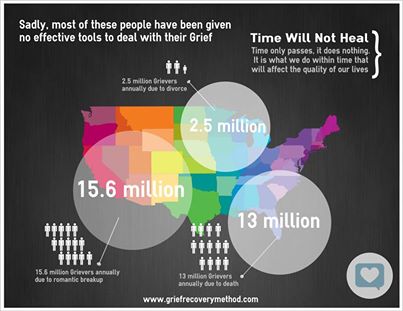
In Part 1, I summarized the Grief Recovery Handbook (GRH) instructions for making a lifetime Loss History Graph; then figuring out which personal relationships dealt us the most of these losses; and then how to write a separate “Grief Recovery Completion Letter” to each of those persons. (“Millions lack tools for Grief,” by the GRH website GriefRecoveryMethod.com)
Complicated? Overwhelming? Sure. But wait – there’s more!
We also need a Grief Partner to join us in doing all this homework. They must meet with us weekly so we can read our homework to each other; and then later read our Grief Letters to each other. This goes on for as many weeks, or months, until we felt we’ve been “seen and heard” enough by another real live human being, to somehow deal with the pain.
“This is why I tell people that God put tear ducts in our eyes,” I read two years later in a book by Dr. John Townsend. “Grief is a relational experience, and your pain has to be seen eye to eye with another person. Someone should be looking at us when we are crying, and we should be looking at him or her. Then we know that we are not alone, and that our tears are seen and heard.”
My pal Steve and I both saw instantly that a partner was key; so we hated to start all that homework without getting leads on partners. What if we got too far ahead, with no one working with us? Now the real “fun” began.
We soon learned that finding a Grief Partner was only slightly less tough than finding a marriage partner — or a unicorn. “Unicorn hunt” became our grim buzzword. We couldn’t work with each other; mourning some details with the opposite sex was too embarrassing. We needed a gal for me and a guy for him.
I went to the local hospice and community groups looking for others in mourning who also needed relief, while Steve asked around at the office and in choir. But it soon became clear that people didn’t like to admit to feelings like this, or if they did, were disposed (as society demands) to minimize losses and “put on a Happy Face.” Last hidey hole: they were “just too busy.”
After two months’ search, at the end of June 2009 I spoke to my local hospice director Greg about my difficulties finding a partner. I was too embarrassed to discuss my Mom’s death due to my horrid conflict with her. The GRH calls this the “loss of a less-than-loved-one.”
“With all these people crying about how they miss their beloved parent, I’m afraid to upset them by discussing my nasty feelings about mine,” I said. “I don’t fit in anywhere, not even here.” “You are not a freak,” he replied. “Just because you have complex grief does not mean you’re an imposition on other grievers.”
Finally I asked Greg, as a professional, to sit and hear me read my Loss History Graph.
The Loss History Graph
On July 3, I took a room at the beach for the summer of 2009 and had at my first assignment, my Loss History Graph. This opener is not about any one person in our lives, but rather a list of all the major losses we’ve ever felt. I didn’t know it, but I fled to the ocean for a reason; this was going to be ‘way too much to take without some sort of natural beauty for comfort. (Another graphic from GriefRecoveryMethod.com)
The exercise blew me away; what I saw was that I’d had an entire life of loss. My emotional pain and losses went back as far as conscious thought — and just kept coming. The graph was assigned to fit on one page, but I needed two and that would hold only my worst losses in my tiniest scrawls.
My first memory was swallowing a penny circa age 4; I’ve related that and other frightening experiences with Mom at age 4,5 and 6 in Chapter 3. At 5 my best friend Helen from next door fell off our swing, broke her arm, and was never allowed in our yard again; I was crushed. At 9, I cracked a lamp and was told I’d destroyed a priceless heirloom. During the Cuban Missile Crisis, cowering under the schools desks I felt somehow way more terrified than other kids and completely alone in the agony.
Then came the JFK assassination which terrified me to the point that for no reason anyone could grasp, I began crying uncontrollably and went on sobbing in my room for weeks. Finally Dad came in and said, “That’s enough now, cut it out.” Mom and he were displeased when I cried and that was the signal to be quiet.
Other than that Dad didn’t appear on the graph. I wrote in the margin “Never home; never told the truth that Mom was crazy, not me; never stood up for me.”
My high school boyfriend Alan left me at 17 saying I was too crazy (now we know he was right). At 18 my first college boyfriend Jim got so depressed when his brother committed a murder, that Jim broke up with me. Being dumped by Jim was my first major prolonged romantic crash; I was completely crushed. I cried and hid in my dorm for a year. No one, led by me, could figure out why my crash was so big; the rejection felt like the earth had fallen out from under my feet. I didn’t actually recover from it for many years; I just kept moving.
At 19 I met my college beau Larry; then I fled to Japan at 21, ended up in medical school in Manila, returned home at 25 and was excommunicated from my family when I quit medicine. The loss of no longer being able to see my sister alone was a mind-boggling amount of agony.
Then I married Larry and had 27 years of loss, starting with an awful abortion in 1982 when he refused to have children. There was no room on the first graph for all the marriage losses; he’d get his own personal Larry Loss Graph and Larry Grief Letter later. Next we lost our international business due to Sept. 11, 2001.
When I finally left our home back east in 2006 and headed to California, I had to add the loss of my house and home, all my friends, my 25-year singing career, my beloved pianist (truly one of a kind), and all my finances in bankruptcy. Next came the losses I took in two nasty rebound affairs.
My jaw dropped as loss after loss spilled out and the large sheets of paper became entirely covered in ever more tiny black scrawls of more and more bad memories until there was almost no white space. Gosh, I thought I’d had such a happy life with all that glorious music and global business travel!
“My heart’s like a car which was totaled approximately at birth, and never got any gas or oil, but I just kept driving,” I wrote. “I’ve driven in the Grand Prix to the moon and back a few times — and now I open the hood, and my engine crumbles onto the asphalt in a pile of rust.” In the Loss Graph margin I scrawled: “Unwanted pregnancy would accept all of this to gain any self-validation as in ‘Yes You’re OK to have been Born.’ Need to prove you had a right to exist, contrary to the message you got.”
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
Footnotes
FN1 James, John W.; Friedman, Russell, “Moving On: Dump your relationship baggage and make room for the love of your life,” M. Evans (Rowman & Littlefield), Lanham, MD, 2006. This is also a terrific book, if you’ve grieved your already huge losses (I hadn’t) and are ready to move on (I wasn’t).
FN2 James, John W.; Friedman, Russell, “The Grief Recovery Handbook,” Harper Collins, New York, 2009 (orginal 1998)
FN3 James, John W.; Friedman, Russell, “Pay Me Now or Pay Me Later,” www.grief-recovery.com/Articles/Pay_Me_Now.htm, The Grief Recovery Institute, 2002
FN4 Townsend, John, PhD; Cloud, Henry PhD, “How People Grow,” Zondervan, Grand Rapids, MI, 2001
The “Grief Recovery Handbook” by John James and Russell Friedman is an invaluable tool for healing emotional pain and loss. It saved me after the death of my parents and my divorce, which all happened at once.
It shows us how to write “Grief Letters” to our “dearly beloved,” and read it to a listener. This simple eye contact with another human, who need only be silent and accept our grief, pain, and yes tears, creates astonishing healing. “This is why…God put tear ducts in our eyes,” says Dr. John Townsend. “Someone should be looking at us when we are crying…Then we know that we are not alone, our tears are seen and heard.”
If you’ve lost a dearly beloved, you could just buy 2 copies, find a “grief partner” who’s also had a loss, and follow the book. The grief letters may be straightforward for you, and then you’ll be “complete” and heal. You may not need this blog.
But I had childhood trauma, and neither my parents, nor my ex, were “clearly beloved.” There was a lot of muddy pain and hurt; I was stuck with “the death of a less-than-loved one.” I had to walk a convoluted path to discover how to grieve pain from before consciousness. It got dangerous.
It was March 2009 and my choir car pool buddy Steve was in a sea of emotional pain since his wife’s death; I’d advised him in 2008 to get the “Grief Recovery Handbook” by John James and Russell Friedman. I thought it was about death, which clearly was his issue, not mine. I thought my issue was to replace my ex with a new romance, so I got their other book, “Moving On.” [FN1]
But Steve, ever the engineer, was determined to deal with pain scientifically. He took one look at the book and bought a second copy for me. “This is a program to retrain the emotions,” he announced. “You need it too.” [FN2]
Thus began our three-year saga with the Grief Recovery Handbook or GRHas Steve fondly dubbed it. We wanted off the pain train, and bad.
“A broken heart is like a flat tire. Waiting for time to heal your heart without taking action, is like waiting for air to jump back into a flat tire,” the GRH begins. “That’s what the grief process does. It’s an action we can take… Action first, feelings follow,” it repeats. “Don’t wait to act until you feel better; you’ll never feel better unless you act.”
Most of what you know about emotional pain is wrong, the book next announces — we’ve all been taught Six Myths in particular which are a fraud. These myths make grieving impossible, forcing us to keep carrying the pain around, often for life:
1. Don’t feel bad. (Don’t feel. Feelings are bad. Stuff it.)
2. Replace the loss. (Get a new spouse, just like a new cat.)
3. Grieve alone (Go to your room. Sadness is impolite. You’re bad.)
4. Just give it time. (Just sit; air will spring into the tire.)
5. Be strong for others. (Your feelings aren’t important, nor are you.)
6. Keep busy. (Distractions help us to stuff it.)
Pay Me Now or Pay Me Later
In a brilliant article “Pay Me Now or Pay Me Later,” James and Friedman compare the heart to an auto engine. It’s an imperfect world, despite the fantasies of perfectionists, so loss and hurt often start at an early age. “You might recognize the title from an advertising slogan for an automotive product several years ago,” they write. The idea was that if you spend a little money on maintenance now, you might save a tremendous amount replacing an entire engine later. [FN3]
“In the auto commercial it was failure to change the oil filter which led to a build up of crud, which clogged and eventually destroyed the motor. Thus, buy an inexpensive filter now or buy a whole new engine later.”
As we go through life, they say, stuffing when we’re hurt instead of grieving, this “crud” builds up around our hearts and thickens year on year. “Grief is negative, and cumulatively negative,” they say, in a key insight.
Then a serious tragedy hits, like a death or divorce, and we don’t realize it, but it triggers all those past hurts we never grieved. Our hearts are breaking inside – but our heart is so hard outside, due to the thick crud, that we can’t see out, so we go into a tailspin.
Now we’re in big trouble and with decades of crud around our hearts.
What to do? Grieve today’s loss thoroughly; that may also help grieve the past, they advise. “Right after a loss, we have a direct pathway to our experiences in the relationship,” they say. “Death and divorce both tend to trigger memories about the emotional aspects of relationships that may never have been communicated about or completed…
“But as time elapses those memories are more difficult to access,” so we’ve got to start now. Otherwise “the build up of emotional ‘crud’ around the heart almost automatically tends to cause us to limit or restrict the kind of interactions that require an open, loving heart.” We become unable to really relate to “safe” people, so we only find more bad relationships.
Grief Letters, Grief Partners
What about action? You asked for it. [Something’s wrong with my software; click on image at right of my 2009 cartoon “Flatten Me” to see it.]
The GRH details actions which are concrete, detailed, extensive, and time-consuming — i.e., credible, and scary as hell. We’d need to make a Loss History Graph detailing the major losses of our entire lives; determine which two or three personal relationships entailed the most losses; and then write a separate “Grief Recovery Completion Letter” to each of those persons. ( p145)
We start with the individual about whom we feel the most pain, and make a Relationship Graph of the major losses related specifically to them.
Next we abstract the incidents on the individual’s Relationship Graph into Recovery Components for that person. Then we turn the Components into a Grief Recovery Completion Letter (Grief Letter hereafter) to that person — and read it aloud.
Then we repeat all those steps separately for each other individual in relation to whom we’d felt significant loss or pain! Doing all this was going to take a big bite out of our lives, and we whined about it up front: Good Grief, Charlie Brown.
Complicated? Overwhelming? Sure. But wait – there’s more!
Stay tuned for Part 2…
Can’t wait? Here’s the whole thing: http://attachmentdisorderhealing.com/featured-topics/grief-recovery/
——————
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
Footnotes
FN1 James, John W.; Friedman, Russell, “Moving On: Dump your relationship baggage and make room for the love of your life,” M. Evans (Rowman & Littlefield), Lanham, MD, 2006. This is also a terrific book, if you’ve grieved your already huge losses (I hadn’t) and are ready to move on (I wasn’t).
FN2 James, John W.; Friedman, Russell, “The Grief Recovery Handbook,” Harper Collins, New York, 2009 (orginal 1998)
FN3 James, John W.; Friedman, Russell, “Pay Me Now or Pay Me Later,” www.grief-recovery.com/Articles/Pay_Me_Now.htm, The Grief Recovery Institute, 2002
I went through three bad therapists before I found my current one, and for the first two years, I kept asking him the same question: “You’re just a hired gun, right? ‘What’s love got to do with it?’ What good can this really do me, since it’s just business?”
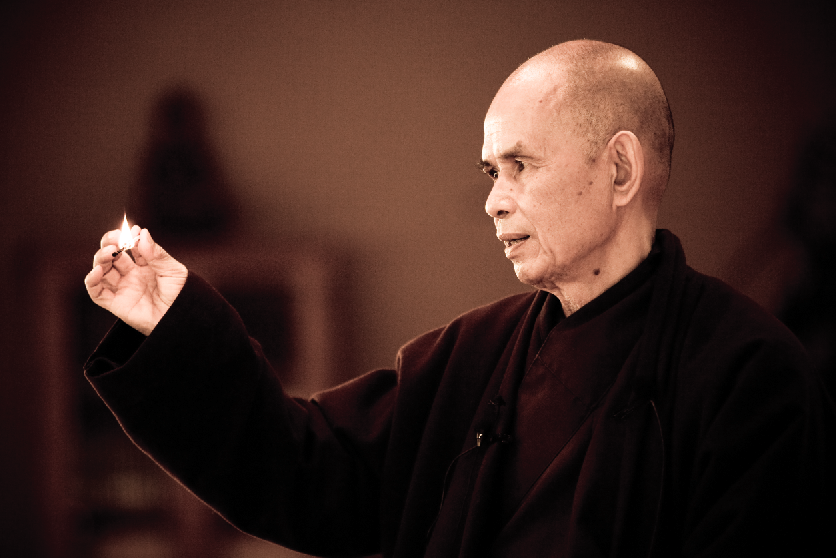
Then one day I was reading Thich Nhat Hanh’s “The Heart of the Buddha’s Teaching” (photo above by PlumVillage.org). On page 5, Nhat Hanh writes this of his youth in Vietnam: “I grew up in a time of war. There was destruction all around – children, adults, values, a whole country. As a young person, I suffered a lot. Once the door of awareness has been opened, you cannot close it. The wounds of war in me are still not healed. There are nights I lie awake and embrace my people, my country, and the whole planet with mindful breathing…”
I dissolved in tears, that such a leader of men could live with this terrible pain.
Then he says: “Please don’t run away from your suffering. Embrace it, and cherish it. Go to the Buddha, sit with him, and show him your pain. He will look at you with eyes of loving kindness, compassion, and mindfulness, and show you ways to embrace your suffering and look deeply into it. With this understanding and compassion, you will be able to heal the wounds in your heart…”
Just as suddenly I flashed on a picture of my therapist, grey beard and all. Whoa, he’s a Christian therapist, and I’m (or was) a nice Jewish girl from Long Island — so “trust me,” as we say in New York, Dr. R. was thefurthest thing from my mind when I picked up Nhat Hahn’s book.
But now it hits me like a ton of bricks:
“Oh: Buddha!,” I said, speaking mentally to Dr. R. “This is how you look at me, this is how you create deep changes in my soul…” And then I was really bawling and calling Dr. R’s tape to leave a message reading him Nhat Hanh’s passage — saying, more or less, “OK, now I get it! This is real attachment, it’s the real deal! Hey, Buddha…”
In the years since, we’ve discussed it, and lived it, and he says it — but now I knew: Dr. R. is 100% invested in me.
Not the way he’s invested in 40lks or in paying his mortgage; he could make a living an easier way. Instead, he chooses to invest his emotions and attachment into his clients as a dear friend would. He chooses to lay his soul out under me like a warm limbic carpet of deep emotional support, as Sir Walter Raleigh did his cloak for Queen Elizabeth.
That takes courage and ginormous simply plain human compassion and sheer humanity.
Recently I read these words by Sir Richard Bowlby, son of the founder of attachment theory, addressing therapy for adopted children — but it goes for anyone who needs deep therapy, and it made my whole body sob:
“The… intervention …involves clinicians taping into their own empathic capacities to help children feel supported to such a degree that direct connections can be forged between the reality of children’s traumatic experiences and the parents and/or clinicians being able to tolerate their pain and so regulate the child’s distress down to a manageable level. The recognition that another person can truly understand and tolerate their pain can be a major contribution to the client’s therapeutic outcome. ” http://www.beyondconsequences.com/bowlby.html
If you consider the level of pain that I get into with developmental trauma since the sperm hit the egg, Dr. R. is tolerating hell on wheels – and that is because he did not shrink (ooooops, bad pun) from the only way to gain that skill: he has looked deeply within himself in years past, and he has done his own trauma healing as deeply as he’s asking me to do.
[This post originated when I saw a comment on an article by therapist Dr. Laura K. Kerr, in which the commentator felt that therapy can’t be more than a business transaction; original at: http://www.socialjusticesolutions.org/2015/04/01/trauma-informed-psychotherapy-puts-body-love-back-mental-healthcare/#comment-125547]
“General Theory” on Therapy and Love:
The psychiatric text “General Theory of Love” shows that human beings depends for survival on our mammalian “limbic brain,” and that as we grow, our minds and souls are healthy and feel well, or don’t, depending literally upon love. [FN1] (Click on graphic to open; from Boise State University News.)
It also documents that good therapy is nothing but love. The problem, they point out, is that too many therapists can’t manage that kind of good therapy.
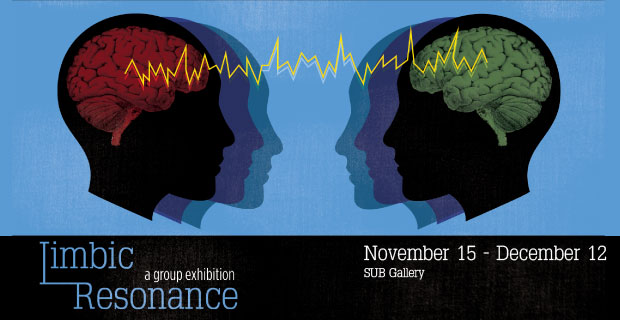
Our caregivers create our infant brain via “limbic resonance,” they report, the resonating of an adult’s limbic brain with an infant’s limbic brain — via attuned deep eye contact. “By looking into his eyes and becoming attuned to his inner state, a mother can intuit her baby’s feelings and needs,” they write. “The regular application of that knowledge changes a child’s emotional makeup.”
When the mother attunes to the infant with deep love, the infant learns that love is safe, forms a secure attachment, feels a sense of belonging and a sense of peace. “Attachment penetrates to the neural core of what it means to be a human being” they write, and thus the book’s title. It’s all about love and nothing but love. More details: http://attachmentdisorderhealing.com/love-theory-2/
The book’s second half demonstrates that psychotherapy works when it does, only due to love — love precisely of the above deep nature. And therapy doesn’t work when limbic resonance and love don’t flower. It’s got nothing to do with a charity date or even such foolishness as “re-parenting.”
It’s just plain and simple deep human compassion, eye to eye. For that reason, “psychotherapy is physiology,” they state.
“When a person starts therapy… he is stepping into a somatic state of relatedness, ” they report. “Evolution has sculpted mammals… (to) become attuned to on another’s evocative signals and alter the structure of one another’s nervous systems. Psychotherapy’s transformative power comes from engaging and directing these ancient mechanisms. Therapy is a living embodiment of limbic processes as corporeal as digestion or respiration.
“Speech is a fancy neocortical skill, but therapy belongs to the older realm of the emotional mind, the limbic brain.
“Love is not only an end for therapy; it is also the means whereby every end is reached. (p.168-9) The first part of emotional healing is being limbically known – having someone with a keen ear [a good therapist-kb] catch your melodic essence.” (p.170)
Unfortunately there are a lot of incompetent therapists hiding behind their desks and diplomas, refusing to really relate. “Some therapists recoil from the pivotal power of relatedness. They have been told to deliver insight — a job description evocative of estate planning or financial consulting, the calm dispensation of tidy data packets from the other side of an imposing desk,” writes “General Theory.”
“A therapist who fears dependence will tell his patient, sometimes openly, that the urge to rely is pathologic. In doing so he denigrates a cardinal tool. A parent who rejects a child’s desire to depend raises a fragile person. Those children, grown to adulthood, are frequently among those who come for help.
“If patient and therapist are to proceed together down a curative path, they must allow limbic regulation and its companion moon, dependence, to make the revolutionary magic.
“Many therapists believe that reliance fosters a detrimental dependency. Instead, they say, patients should be directed to “do it for themselves” – as if they possess everything but the wit to throw that switch and get on with their lives.
Limbic Revision
“But people do not learn emotional modulation as they do geometry or the names of state capitals. They absorb the skill from living in the presence of an adept external modulator, and they learn it implicitly,” the book states. ” Knowledge leaps the gap from one mind to the other, but the learner does not experience the transferred information as an explicit strategy. Instead, a spontaneous capacity germinates and becomes a natural part of the self, like knowing how to ride a bike or tie one’s shoes.” (p.171) (graphic by N.Bam on Tumblr)
“People who need regulation often leave therapy sessions feeling calmer, stronger, safer, more able to handle the world. … The longer a patient depends, the more his stability swells, expanding infinitesimally with ever session as length is added to a woven cloth with each pass of the shuttle, each contraction of the loom. And after he weaves enough of it, the day comes when the patient will unfurl his independence like a pair of spread wings. Free at last, he catches a wind and rides into other lands.” (p.172)
“Knowing someone is the first goal of therapy… Therapy’s last and most ambitious aim is revising the neural code that directs an emotional life. (176) Psychotherapy changes people because one mammal can restructure the limbic brain of another… (p.177)
“Describing good relatedness to someone, no matter how precisely or how often, does not inscribe it into the neural networks that inspire love. Self-help books are like car repair manuals: you can read them all day, but doing so doesn’t fix a thing.
“Working on a car means rolling up your sleeves and getting under the hood, and you have to be willing to get dirt on your hands and grease beneath your fingernails. Overhauling emotional knowledge is no spectator sport; it demands the messy experience of yanking and tinkering that comes from a limbic bond. If someone’s relationship today bear a troubled imprint, they do so because an influential relationship left its mark on a child’s mind.
“When a limbic connection has established a neural pattern, it takes a limbic connection to revise it. (p.177)”
“The person of the therapist is the converting catalyst, not his credo, not his location in the room, not his exquisitely chosen words or silences… The dispensable trappings of dogma may determine what a therapist thinks he is doing, what he talks about when he talks about therapy, but the agent of change is who he is. (187)
“The brevity of mini (psycho)therapies is another efficient forestaller of healing. The neocortex rapidly masters didactic information, but the limbic brain takes mountains of repetition. No one expects to play the flute in six lessons or to become fluent in Italian in ten. ” (p.189) “The skill of becoming and remaining attuned to another’s emotional rhythms requires a solid investment of years.” (p.205)
“The limbic connectedness of a working psychotherapy requires uncommon courage. A patient asks to surrender the life he knows and to enter and emotional world he has never seen; he offers himself up to be changed in ways he can’t possibly envision. As his assurance of successful transmutation he has only the gossamer of faith…
“Only human love keeps this from being the act of two madmen. (p.190)”
———————————
Kathy’s news blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
In 2013 I began working with Sandra Paulsen, PhD. I am very grateful for the early childhood trauma (ET) work we did. It was a stunning process that gave me understanding and resolution of significant traumas. I learned to understand “ego states” and gained a view of the numerous parts of me that acted as protectors throughout my life. The use of “the conference room” was difficult and surprising at first, but with Dr. Paulsen’s encouragement and compassion for “the little one” inside me, it quickly became easier for me to imagine a conference room in which I could see “parts of my self” sitting around a table.
We worked intensively in long sessions often using EMDR therapy. The tappers were scary sometimes, but became easier for me to tolerate; they create a mild, alternating bilateral vibration and can be held. [EMDR therapy for ET may tap on alternate feet or other areas away from the face, rather than moving a finger before the eyes as in Francine Shapiro’s original EMDR therapy. -kb]
Initially, I learned to ground myself in the present where I felt safe. Within a short time, I was able recognize parts of self in the conference room, an imaginal place in my mind’s eye where different aspects, or parts, of myself could come to help us understand and access trauma memories. The process revealed difficult memories that enabled me to understand “the why” of my lifelong struggle with confusing fear, along with the “why” I felt a need to isolate myself from family and friends.
At the end of each session. the content of our work was consciously set aside in an imaginal “vault” in the conference room until next time. I envisioned my memories and feelings floating down a stream into a large container that held them tightly (the vault). After most sessions, despite my recall of terrifying memories, anger, and tears, I felt relief. Thinking of those sessions now, I’m amazed by the sense of safety I felt with Dr. Paulsen.
Developing Confidence, Deep Body Memories
I developed confidence in the process and believed that one day my “whole self” would be healed. I realized too that I was becoming valuable to myself for the first time. [Sandra Paulsen, right]
I remembered more than I could have imagined. Often my body felt memories first. These somatic memories led me through a long trail of abuse and abandonment by family members. Remembering specific parts of the abuse was a surprise at times. I attribute the lack of memory to my amnesia barrier and am grateful that my brain was able to develop the barrier. I sometimes recall those surprising memories and marvel at the function of our brains.
I’m also grateful that Dr. Paulsen took time to help me build boundaries that I could use then and later to further process my memories. My new boundaries were a great help in painful relationships, which could have destroyed my fragile but growing sense of self.
When visualizing my childhood “parts of self” with Dr. Paulsen, I began to appreciate each part and welcomed the knowledge we recovered together. My parts worked together to accept the reality I could not manage to be aware of in childhood. I love knowing that my unconscious mind protected the conscious me and built a complex support system. My understanding and knowledge of my parts is pivotal to release, resolution and healing of my fragmented self.
I am learning to accept all of me rather than just “the parts” my family wanted. The good and bad parts held me together in the midst of chaos. I’ve decided the difference between some of the “good and bad” parts of self were those behaviors or beliefs that were acceptable or not.
My experience taught me that I was never safe in my family because attitudes could change in a moment. I lived in fear of the unexpected changes and surprise attacks. Sometimes it’s difficult to like certain parts because I viewed them as causing the pain of disapproval and abandonment. In reality, my unacceptable parts were protecting me.
After working with Dr. Paulsen, I understand the functions each had in helping me stay alive. For instance, I have a split sense of God. I’ve hated the bad God part (judgment) and love the good God part (compassion). I understand now that “bad God” part protected me from my family because “bad God” taught me to act the “right” way. To understand it now is valuable, but the judgment led to self-loathing. It’s amazing that hating myself made me safer within my family. All I could expect was abandonment and a family that used me rather than caring for me.
My feelings about my family are still confusing, but I’m learning to view them from a distance. My mother and father are not bad. There were reasons for their behavior. I am aware that I see them as the bad parts who inflicted pain. I expect that resolution can be reached in time.
I developed the ability to talk with my parts. We have safe spaces to talk, reflect and empathize with ourselves. I’ve found this essential. The spaces are in nature…a forest, the beach or a quiet space for meditation. Walking in a peaceful place is important to clearly see our existence together and care about our efforts toward wellness.
Anger, Move to Chicago
On the opposite side of the peaceful place is the angry place. It’s very difficult for me to acknowledge anger at others because it is dangerous to do so. Working with Dr. Paulsen, I could acknowledge the anger. My acknowledgment of angry feelings was hard because I was not able to express it in childhood or even in adulthood. For me anger is the most dangerous feeling. Others could be angry with me, but I could not express anger toward them. Our work helped release some of my angry feelings, but it’s still difficult to feel safe enough to express angry feelings appropriately. I recognize the angry parts of self. I think we’re still waiting to feel safe and valuable enough to own those feelings. I continue to work in my messy angry part of self.
In April 2014, I met D. Michael Coy, MA, LCSW [above], to whom I was referred by Dr. Paulsen before I returned to live in the Chicago area. As it was with Dr. Paulsen, our work together has focused on my dissociated “parts of self,” but now using EMDR and other therapies to focus on the later memories of traumatic experience that I continue to struggle to get past.
Looking back over my time since I began working with Dr. Paulsen, then with Michael Coy, I’ve watched myself grow. I care for the many dissociated “parts of self.” Visualizing my “parts of self,” I understand how each developed and the job each part did to prevent damage throughout my life. I love knowing that my unconscious mind always protected me. My understanding and knowledge of my parts is pivotal to release of trauma on every level. I expect to function in the months ahead as the “whole person” I am.
In summary… there is so much more to know and say about living with (and healing from) complex trauma. It’s a relief to know that my symptoms are real and not made up. I cannot express my relief in light of my work in the therapeutic process called the EMDR early trauma approach, which Dr. Paulsen has so skillfully developed further to work with people like me, who struggle with complex traumatic experience. I can honestly say that I’ve never been more hopeful in my life.
———————————
Kathy’s blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
Footnotes
FN1, “Neurobiology and Treatment of Traumatic Dissociation: Toward an Embodied Self,” by Lanius, Paulsen, and Corrigan, 2014, http://www.amazon.com/Neurobiology-Treatment-Traumatic-Dissociation-Embodied/dp/0826106315
See also especially Dr. Paulsen’s website: http://www.bainbridgepsychology.com/EarlyTraumaOShea.html
Guest blog by Dr. Sandra Paulsen (left) & D. Michael Coy, MA, LCSW
[First I discovered it deep within myself and called it “trauma since the sperm hit the egg.” Then I read that Bessel van der Kolk calls it “developmental trauma,” in his drive to have it finally recognized by the psychiatric profession. Dr. Allan Schore calls it “trauma in the first 1000 days, conception to age two.” Earlier it was “complex PTSD” or C-PTSD. In EMDR therapy, Dr. Sandra Paulsen, therapist Katie O’Shea, LCPC (who began this work), and D. Michael Coy, MA, LCSW, use “Early Trauma” (ET). The science is in Chaps. 16 & 20 of Paulsen’s 2014 book. [FN1]
[Well: “ET, phone home!” Dr. Paulsen & friends have good news: they’ve created new EMDR therapy protocols to heal developmental trauma. -kb ]
Eye Movement Desensitization and Reprocessing (EMDR) therapy “enables people to heal from the symptoms and emotional distress that result from disturbing life experiences,” says Dr. Francine Shapiro’s EMDR Institute website. Standard EMDR therapy has been shown to heal traumatic memories with a conscious, visual component, also called “explicit” memory. As EMDR clinicians, we have seen frankly astounding changes in our clients, both in how they see themselves and in how they experience and take initiative in the world.
But with in utero and infant Early Trauma (ET) occurring from conception to age three, also called developmental trauma, there is no conscious, explicit narrative memory — infants have not developed the parts of the brain which can think. These traumas precede the existence of consciousness, so they’re called pre-conscious or “implicit” memories. Such memories are “somatic,” that is, held purely in the body — so healing is far more challenging.
How can we listen to the unspoken experience when, so early on, there were no words to tell it? How can we help the body tell its silent—or silenced—story?
Limitations of EMDR Therapy Standard Protocols
Sandra Paulsen and colleague Katie O’Shea (right) observe the limitations of standard EMDR as applied to early trauma, specifically:
1) There is no explicit memory in the first years of life, only implicit memory, so the standard EMDR procedure of targeting a memory of trauma could not apply;
2) If a client were able to access early experience in EMDR therapy, it could easily be overwhelming, without adequate preparation;
3) Early experience, when accessed, also accesses the client’s “felt sense” from that early time, with all the limits of self and inner structure that went along with pre-natal, infant, and early childhood developmental stages; [FN1]
4) Because of the paramount importance of relationship and caregiver attachment in infancy, the processing of early experience via EMDR therapy required modification to ensure the client had the felt sense of the therapist’s compassionate and attentive presence; and,
5) Because very early experience is ephemeral and does not consciously register as pictures or videos (as later memories may), the new EMDR therapy needed to explicitly accommodate the subtlety of infant early processing.
For these reasons a four step protocol was developed, starting with the work of therapist Katie O’Shea, who later brought it to the attention of Sandra Paulsen. They then worked to make these new ideas coherent with the latest neurobiology research by Jack Panksepp, Allan Schore, Daniel J. Siegel, et. al.
Four Steps of the Early Trauma (ET) Approach to EMDR Therapy
Early Trauma reprocessing includes the following steps to provide remedies to the limitations of standard EMDR therapy approaches above. NB: There is substantially more to the treatment than described in this brief summary.
1) Cultivating structured containment of all experience yet to be “learned from or sorted through,” to leave a clear “emotional desktop” for work to occur;
2) Developing a felt sense of safety as a starting point for the work, which is achieved by tapping into and strengthening a naturally occurring (but sometimes hidden) “safe state” in the body. Both steps 1 and 2 may require client practice outside of therapy sessions;
3) The most mysterious step—resetting the affective circuits—involves clearing the emotional pathways that develop in each of us early on during our development in the womb, but which may be congested from maladaptive early learning and inhibitions about whether emotions are okay and safe. Once the circuits are clear, they can function as they were intended, to conduct emotional information between the brain and the body. This step may work directly on subcortical affective circuits, according to Jaak Panksepp in his groundbreaking book, Affective Neuroscience. For individuals with complex trauma histories and/or emotional dysregulation and imbalance, there may need to be additional preparation, most commonly ego state work; further education about healthy emotion, brain functioning and/or trauma; sometimes somatic work; and,
4) Clearing the early trauma, which happens by processing small time periods, beginning with a time before conception (owing to what is theorized to be generational, cellular memory), then moving on to conception, gestation in the womb, birth, and on through the first few years of life. These time periods are variable with the client, depending how “gnarled” the roots of the tree have become by growing around early obstacles. The clearing may be of somatic/implicit memory or of explicit memory, or mental constructs related to the time periods. For each time period, if it doesn’t resolve spontaneously, there is an imaginal good outcome of “what you needed, the way you needed it to be.”
As noted, there is much more to it, but for many the careful application of these steps produces a critical emotional shift with subsequent increase in emotional stability, comfort, and peaceful relation to one’s emotions and the self.
The Mechanics of the Early Trauma Approach
The experience of the infant is almost entirely a “felt sense,” as there is not much cognition at the beginning. So when therapy taps into those early felt senses, it often occurs without as the access to the more conscious and cognitively informed resources usually available to adults. Because of its central role in early life, this felt sense is an ideal entry point for attending to early, emotionally overwhelming experience so that it can be reprocessed and cleared.
As we are relying upon the most primitive information available to reprocess early experience, the standard EMDR therapy modality of eye movements or taps conducted with equipment may be too scary, too technical, and too alienating for some. Therefore, the reprocessing is facilitated by tapping on the client’s ankles, while the client is sitting back in a comfortable, reclining chair.
Because processing may occur over a period of hours, people often want to take off their shoes. This certainly makes it easier to tap on the ankles, and is mentioned here because people sometimes wish they’d worn different socks!
Early trauma reprocessing is designed to come in from the beginning, ‘under the floor-boards’, so to speak, so it is typically quite gentle and tolerable in comparison to consciously-focused EMDR therapy. Grounding is needed much less than in standard EMDR therapy procedures. People learn a lot about their own story in this lovely and very powerful procedure.
Highly-dissociative people are only appropriate for this method if they have already established considerable groundwork in therapy and there is a self-system to allow the work. The early trauma therapist ideally is experienced in working with dissociative clients and addressing concerns protective parts may have, as this piece is critical to ensuring positive outcomes in early trauma resolution work. If a potential client is dissociative and, after the initial evaluation, the early trauma therapist agrees to work with the client using the EMDR early trauma approach, it is necessary that the client have an ongoing therapeutic relationship to receive them after leaving the intensive work, assuming that the client is not working with the early trauma therapist in an ongoing treatment relationship. When the client has a primary therapist, it is typically necessary for the client to grant written permission for the early trauma therapist to collaborate with the primary therapist before and/or after the early trauma work takes place.
Intensive or Week by Week Treatments?
Although early trauma reprocessing can occur piecemeal, from week to week, hour by hour, this can be both terribly inefficient and not particularly cost-effective. The ideal way to experience this type of reprocessing is in extended, face-to-face sessions. Because the work is subtle, deep, and more felt than thought about in a conscious way, extended sessions allow the work to unfold viscerally and deeply. It’s akin to being on a commercial flight from Chicago to Minneapolis versus a flight from Chicago to Tokyo: yes, you get somewhere in both cases, but if you’re on the long-haul flight, you’re up in the air longer, you move more quickly, and your fuel efficiency is significantly better.
Notably, the Dr. Paulsen uses the intensive approach exclusively. In some instances where there is an ongoing therapy relationship, and insurance coverage is involved, the early trauma therapist and client may resolve that week-by-week treatment is the only way to go. This is the only option for a number of the clients who see Michael (above left), either because the client is not able to do the intensive work immediately (owing to extended preparation being needed), wishes to use their insurance in order to afford it, or they’d like to do the work in the context of longer-term therapy work.
However, the client should expect that it will take a number of months to complete the process of clearing early trauma. Michael does both intensive and week-to-week early trauma resolution work, as appropriate and necessary. Other therapists experienced in the EMDR early trauma approach likely structure the work in a way that fits the needs of their own practice and clients.
It is not easy to predict whether a client will need one, two, or more days of intensive work to clear the entirety of early disturbances and replace it with a felt sense of well-being. This goal is typically possible, but not necessarily easy to schedule or predict. Most people who have participated in intensives require two to three days, or more, to clear the first few years. The time required is variable, based upon how many traumatic experiences there were, how much neglect there was, and how maladaptive the learning outcomes were from those experiences. (Note that it’s not you as an adult who consciously assesses all of what was traumatic in those early times. Your brain did that for you before you were even consciously aware that any kind of wounding was taking place.)
Is This Treatment Right for You?
As different EMDR early trauma therapists may handle assessment, differently, we will speak here to how we approach it. Diagnostic assessment involves looking with the client at the following factors: 1) the client’s present safety and stability; 2) the client’s capacity for experiencing emotion and body sensation; 3) any internal conflicts that may complicate or block trauma resolution; 3) medical concerns; 4) substance use; 5) any evidence of structural dissociation, which would require additional assessment and preparation prior to embarking on trauma resolution work of any kind.
Biographical assessment is also an important piece of assessment. The biographical assessment covers areas of the client’s history such as work, education, military service, nutrition and self-care, basic family history, spiritual and cultural experience, and so on. Biographical assessment can provide both a helpful ‘fly over’ of the client’s experience, as well as point out the ‘smoke trails’ emanating from the client’s early, unresolved experience.
During and After Early Trauma Intensive/Reprocessing
On the first day of the intensive, the therapist and client ensure that all the necessary preparatory steps have either already been undertaken, or they will begin there in the work together.
It is not unusual for a client to feel ‘drained’ after early trauma reprocessing has taken place. Most people don’t want to do much in the evenings after an intensive session. The work is profound and will take some time set aside for introspection just plain rest.
Self-care is key in this work, so plan on drinking plenty of water, getting plenty of sleep, inviting oneself to dream, eat good food, maybe take some anti-oxidants because the client will be releasing energetic holdings. Fruits and vegetables will be put to good work in reconfiguring a ‘new you’. If the client is traveling from a different time zone, it is recommended that they are taking Melatonin or some other supplement (as approved by their primary care physician, as appropriate) to manage the effects of jet lag.
After the work, the nervous system will be “knitting and purling” for a time, and this is usually gentle and comfortable. Occasionally, if the work was paused in a gnarly hurtful baby spot, the client may feel stuck there. In those instances, the client may need help in person or by phone to move through such a spot.
It is also really important to keep in mind that any unusual experiences during the work or in the time right after the work may be related to the work. One can think of these as ‘vapors leaking up from King Tut’s tomb’. So, for example, if the client’s spouse, partner, or a good friend seems, for whatever reason, suddenly to resemble demon spawn, they are encouraged to consider the possibility that something about the early work has a theme of demon spawn in it somewhere.
Similarly, if it seems to the client that the early trauma therapist is suddenly just like the meanest parent ever, they are encouraged to mention this, because, although it may have a basis in present time (and, for Michael, his dogs might agree, depending on which chew-thing he’s rescued from them that day), we’ll consider that, often those kinds of feelings and perceptions are part of the client’s story, telling itself without words. The therapist and client use
information in the room and about what is happening between them, moment to moment, as clues to that story. Client and therapist become detectives together, hearing the client’s story together, however it seems to want to be heard. The most common unsettling experience after early trauma work is to feel oddly inert or flaccid. This seems to be part of a baby state, as if baby is just sitting, waiting, not mobilized for much action.
Closing Thoughts
We feel honored to do this important early trauma work with their clients. Michael was fortunate to have been trained in the EMDR early trauma approach both by its originator Katie O’Shea and by Sandra Paulsen, PhD, with whom Katie has collaborated to bring it to public consciousness and develop it into a replicable, systematic process for healing early wounding that can be used safely and effectively even in the most complex situations. (Notably, a cartoon book for therapists and clients on the EMDR early trauma is currently in press.)
We consider this work a sacred trust. It is such a privilege to hear the story of the baby within that may never have been told or heard before, except in symptoms or reenactments. The EMDR early trauma therapist’s intention is to help the client review, release and repair very early experience in a way that provides a felt sense of well-being. We encourage our clients to spend a little time before we meet identifying, if they don’t already know, what their highest resource is, and what their relationship is to the spiritual realm. Then we are more able to support the client’s process in a way that makes sense to them, on their own terms. This is the most helpful way we know to repair very early injuries, hurts, betrayals and disappointment.
Sandra Paulsen, PhD, is the founder of the Bainbridge Institute for Integrative Psychology and a leading edge practitioner who has integrated her knowledge of Ego State Therapy, somatic therapies, and EMDR therapy to effectively treat clients struggling with complex trauma and dissociation safely and effectively. Dr. Paulsen accept clients for early trauma treatment in the intensive format but only via therapist referrals at this time. See: http://www.bainbridgepsychology.com/ET-Referring-Clinicians.html
D. Michael Coy, LCSW, LICSW, is a Master’s level therapist in independent practice in Chicago, IL, certified in EMDR therapy and also trained in clinical hypnosis, Ego State Therapy, and essential somatic methods for enhancing trauma resolution work. Michael’s primary focus is with clients who struggle with complex PTSD and/or dissociative disorders. Michael is also a clinical associate of the Bainbridge Institute for Integrative Psychology. For more information about Michael, see https://www.dmcoy.com.
———————————
Kathy’s blogs expand on her book “DON’T TRY THIS AT HOME: The Silent Epidemic of Attachment Disorder—How I accidentally regressed myself back to infancy and healed it all.” Watch for the continuing series each Friday, as she explores her journey of recovery by learning the hard way about Attachment Disorder in adults, adult Attachment Theory, and the Adult Attachment Interview.
FN2 For Eugene Gendlin’s foundational work on the “felt sense,” a term he developed, see Gendlin, Eugene T (1978), Befindlichkeit: Heidegger and the philosophy of psychology. Review of Existential Psychology and Psychiatry 16 (1–3): 43–71.
Dr. Peter A. Levine uses Gendlin’s “felt sense” work strongly in his “somatic experiencing” trauma healing: Levine, Peter A., PhD, “Healing Trauma: A Pioneering Program for Restoring the Wisdom of Your Body,” ‘Sounds True, Inc.,’ Boulder CO, 2005; ISBN 1-159179-247-9
My Neurofeedback Journey, 2 of 2
by Tina Marie Hahn — as told to Kathy Brous
Tina added on July 11: I am experiencing major changes in my brain functioning so fast with neurofeedback, although as of this writing, I have only been doing it for three months. But in six months I seriously don’t think I will recognize myself anymore, and I say that after decades of struggle. I truly recommend checking out neurofeedback, for anyone who has failed all the traditional approaches to trauma. Now back to my journey…
Major Trauma Release
On April 27, it had been about three weeks that I’d been working with the BrainPaint® desktop home neurofeedback machine. I’ve been doing about 1.5 hours of neurofeedback a day. That turned out to be a little too much for me as a beginner, so I gave myself a break the last two days.
After my second “Alpha-Theta” training April 19, I could not stop sobbing during the session, or after — for 4 hours straight. It was cathartic. During the session my body was shaking — like really shaking. It reminded me of Peter Levine’s discussions and the video he has of the polar bear shaking after it was attacked and then later it came out of the trauma. It was incredible. I wasn’t just thinking this poison was coming out of my body — I was feeling it. I was shaking worse than if I had been locked for several hours in a deep freezer…
It really was amazing… I let go of a lot of stuff. I saw that my mother did the best she could. I could see myself letting go of the residual anger.
Then, the anger was replaced with a tremendous well of grief and loss. I realized that I was full of so much grief over what could have been and how my life might have been different if this had not happened to me — how my mother’s life would have been different if she had been able to feel love from her children instead of being so stressed that she allowed the most horrific things to happen to her kids.
I thought about how my brother wouldn’t be psychotic if he hadn’t been hurt so much…. How he could know happiness instead of his constant fear…..
And please know: it might not be good for most people to do this alone, as the title of your book says, “Don’t Try This at Home.” For me, I’ve been working on confronting my childhood for decades, so I have an ability to tolerate this intense experience. But for most people, unless you are willing to take chances and you’re pretty strong, a person might get really shaken up. It would probably be good to have a therapist to discuss what is happening and to process those deeply brain stem based emotions — or a group of healing friends. To have someone with you to support you would be helpful.
I might be doing better if I had a therapist too, but like Kathy I’ve had bad experiences with therapy so my confidence in it is low and anyway I’m in a rural area without much available. But I think many people with severe childhood trauma like me who are considering neurofeedback might want to use it with formal support such as therapy or a support group.
For me, I wasn’t re-traumatized. That is all I want to say for now except I think this is a powerful tool!
Getting More Relaxed
By May 6, I found that we need to give the neurofeedback some time to settle into our brain, let the brain settle into new patterns. That’s why I’m not posting as much: I just don’t feel the need to reflectively respond to everything, and that means everything in general. For someone with trauma, that’s progress.
I have been able to work through my anxiety and though it seems strange, send the emails and make the telephone calls that I need to make but generally procrastinate on. I have been cleaning and organizing. Usually I am so disorganized I am not good at this.
Now I am less reactive. I am certain of it. When talking to others and they say something that would generally trigger me – I might still become triggered but there is more of a second or two to contemplate first.
I stopped doing several hours of neurofeedback per day. I think so much was making it very confusing for me to determine what was going on in my brain. While I think generally it has all been effective, I like the general stabilizing non-linear protocol I began with. I have done several more sessions of the “Alpha-Theta.” That is the type that has the capability to take us into the deep meditative state.
I haven’t had anymore of those really emotional spells during the “Alpha-Theta,” but my dreams have been more colorful. Actually last night I had the first dream in color and it was sad, but more positive. Usually my dreams have always about big mean things trying to kill me. So that is great, too.
I feel like I am better able to sit back, take in others point of view, back off from feeling like I have to do everything myself. I really feel this is great. I also attribute it to the neurofeedback. I feel like I could talk to people much easier now and have a great interactive conversation without feeling strange and out of place inside. This is all awesome to me.
And I am feeling like moving into other areas of healing like meditation which I am not good at because of a “way too busy mind that is always quadruple tasking”. I actually sat down and did about 15 minutes of sitting meditation yesterday and that was good. So I think all in all this has been a very positive process for me.
I have also been taking others suggestions or at least listening and then making I think more informed decisions based on information from others. To me this is the start of trying to connect.
Also, though I don’t use Facebook much, I have been posting on Facebook more recently and will see people I know. Before, I would be afraid to send a friend request — I would be too afraid because I’m a bad person, that person wouldn’t want to be my friend. But now, I have been taking chances, sending friend requests and guess what – people have been accepting. I just find this totally weird for me. I don’t look out of control outside but now, I am starting to feel more competent instead of “out of control inside.” By that I mean that strange anxiety when you feel like you don’t belong, like you are an alien to a foreign species. But now I’m starting to feel I do belong more, I’m feeling more human.
A Breakthrough or Epiphany?
On June 8, I wrote that I haven’t posted on my use of the BrainPaint® neurofeedback system for a month for a few reasons.
Good reasons: I felt so much better due to neurofeedback that I got too busy! I’ve been out a lot, creating and attending meetings about the ACE Study and regional trauma-informed schools, and I’m writing several articles. I’ve begun working on key things I used to procrastinate on, that’s also getting better with neurofeedback… I can feel a real improvement in my impulse control and affect regulation (my ability to regulate my emotions is growing nicely.)
I still feel neurofeedback benefiting me in daily activities, for example if I want to write something that makes a point, I do it so that it’s not impulsive, and is worth reading. My new ability to do that is part of the neurofeedback.
But I also missed a lot of BrainPaint® sessions. On the one hand, we do need time for the neurofeedback changes to settle into our brain. But I got 2-3 weeks behind so let me note: For anyone who decides to do home neurofeedback, it is important to follow the BrainPaint® policy to rate your goals and answer the assessment questions before each session, and also be careful to keep up with the updates they issue to their computer system.
I got behind on that because my cursor wasn’t working properly, I was blaming myself, so I missed a lot of sessions. Finally I called my BrainPaint® home neurofeedback coach and we learned it wasn’t my fault — the program needed an update, so it was updated June 5.
Then we reviewed and updated the BrainPaint® assessment together that calculated new protocols and she told me to stop trying to do everything on my own, to please call for help. I promised to follow the directions and did so over the weekend and — wow, did my brain move with the new protocols the system created!
In fact, as I was doing my session with the directed protocols, I came to what I have to call an epiphany. Something has happened to me which feels weird, in fact it feels absolutely crazy (compared to how I used to feel).
I want to report it because it must be the neurofeedback which is really helping me. OK:
I’m often scared to take my dogs to the vet because the office is on a main highway, and the dogs jump out of the car as soon as a door is opened. I’ve been afraid one would jump out and get hit by a car. I have to put them in the back of the RAV4 when driving or I get a 60 or 45 pound dog in my lap, but I couldn’t get them out the back door due to trouble with the auto-lift gate.
Now yesterday while I was doing neurofeedback, for the first time in my life it hit me: Hey, I could go inside the vet’s office and simply ask a front desk person to help me so my dogs don’t jump out and get hurt. This sounds so stupid but it isn’t — it means for the first time in my life I considered asking another person for reasonable help!
That means believing people are supposed to help each other and that some people can be approached for help.
That’s a first step in trust. Amazing.
So I began to weep, really weep.
Let me explain why this feels so weird and crazy and amazing to me.
As many of us with a high Adverse Childhood Experiences (ACE) score, people have horribly hurt me. I’ve come to feel, I want no part of mammalian attachment to people (you call that “fur”) — even if it is the only way to heal. Trusting people is horribly scary for me for reasons like this:
When I was 7 or 8, I was with my dad in the car about an hour away from our trailer. I never asked my dad for anything because he was incredibly mean. My dad smoked in the car with us kids inside. But on this winter day, I had a cold, and as he is smoking, I suddenly couldn’t breath. I am scared to death because I cannot breath. I timidly ask him “Dad could you please stop smoking? I cannot breathe.” His response was “If you don’t like it, I can drop you off here right now and you can walk home!” A very typical response. I don’t know how I managed to escape with my life in that small car for an hour as he puffed away while I was close to respiratory arrest… but I never forgot the incident or the horrible insensitivity.
From that time forward, I could not ask for anything reasonable – I could not ask for something reasonable to save my life.
To others, asking for assistance may seem like a no-brainer. But for me, tremendously hurt by my parents for years starting at a young age — to consider in the middle of today’s neurofeedback session that I could ask the vet for reasonable help — it made me weep.
And I’m going to try to no longer react immediately, even to such epiphanies, as I want to be more reflective going forward — another amazing plus of neurofeedback. But wow, I have experienced an amazing movement of my brain that I don’t think could have occurred any other way.
I may even be able to move to where attaching to people becomes okay.
Oh and as I had this epiphany – my dogs ate my dinner and I didn’t get mad!
———————————
Kathy’s blogs and Guest Blogs explore the journey of recovery from childhood trauma by learning about Adult Attachment Disorder in teens and adults, Adult Attachment Theory, and the Adverse Childhood Experiences (ACE) Study.
My Neurofeedback Journey, 1 of 2
by Tina Marie Hahn — as told to Kathy Brous
I am Dr. Tina Marie Hahn, MD, advocate for Trauma-Informed Care and Communities, and survivor of actually ten Adverse Childhood Experiences (ACEs). As a pediatrician, I screen parents and children alike for childhood trauma. That’s me at 30 months old and my background story is here: http://acestoohigh.com/2014/05…-her-ace-score-is-9/
I’ve been excited for some time to try neurofeedback, after listening to a talk given by Dr. Bessel van der Kolk and Sebern Fisher and reading Dr. van der Kolk’s latest book “The Body Keeps the Score” and a blog on Sebern Fisher’s work with neurofeedback here at http://attachmentdisorderhealing.com/neurofeedback/ I then read three books on neurofeedback, including Dr. Fisher’s book “Neurofeedback in the Treatment of Developmental Trauma: Calming the Fear-Driven Brain” and decided to research several electronic neurofeedback systems for home use.
I report as a user/patient, not as a doctor or expert, because my experience so far has been fairly stormy — I’m just starting out, so I don’t know where this will go and I am not an expert. I feel I should warn readers: if you have experienced severe infant and childhood developmental trauma as I did, neurofeedback seems like a very rewarding method for healing — but it has intense risks if not done with care.
Please if possible, as Kathy’s book says: “Don’t Try This at Home.” Neurofeedback is designed to be done in a trained practitioner’s office. So for most people with trauma, probably it’s best not to do neurofeedback alone at home. Please try to do it with access to formal support, hopefully a good attachment-based psychotherapist who is very compassionate, so you can discuss what is happening and process these deeply brain stem based emotions with another human. If therapy is really impossible, maybe you could create a group of healing friends or at least have a friend come regularly to be with you while you do it or afterward. Some type of support would be key.
I had to opt for a home-use neurofeedback system because I am in a rural backwater where everyone knows everyone so I don’t feel comfortable sharing incredibly strong emotions. I’ve also had prior bad experiences with psychiatry plus right now there aren’t good practitioners anywhere near where I live. In fact, I might be doing better if I had a well-trained therapist possessing extensive knowledge of developmental trauma.
As to the level of pain in my healing with neurofeedback so far: I have been working on this level of emotional pain for decades, so (thus far) it seems I have an ability to tolerate this intense experience. (I won’t know how much I can tolerate until I go further, who knows.) But I did want to note that unless a person is willing to take chances and is pretty strong, they might get really shaken up.
The Fear-Driven Amygdala
I wanted to specifically treat my fear-driven amygdala that I have from being terrorized as an infant and child. I found one home system, which looked good, but it did not allow one to use different protocols to specifically calm down an overactive amygdala.
So I chose BrainPaint®, which did, and I was excited to get my BrainPaint® home neurofeedback system in the mail April 6. BrainPaint® sent an excellent 47 minute video tutorial showing me how to set up the system and before the first session, I had an 1.5-hour phone tutorial. The system is very easy to set up and use. Also we get 45 minutes of assistance by phone every month we rent the system, and we can pay extra for more telephone help if we need it. I will be texting or calling my BrainPaint® “assistant” to help me as I become ready to change protocols based on symptom improvement.
BrainPaint® is not cheap but mental health and well-being? Priceless. The BrainPaint® set I got has a minimum two months rental at $675 per month for shipping and a deposit; I initially paid $1,875. The deposit comes back when you send the rental back. Here is an introductory YouTube video: https://www.youtube.com/watch?v=7s0AFjRVfmk
I did my first session April 7; it starts with a symptom checklist. I had lots of symptoms checked. The protocol chosen initially was to calm my right amygdala— but because it looked like so many areas were out of whack, I did something called “non-linear on T3 and T4″ (right and left temporal) to get the brain hemispheres in synch.
My first session was 7 minutes….. It was interesting.. Looking at a screen with fractal patterns and auditory inputs. After the first 7 minutes, I fell asleep for 2 hours. For me that is amazing because I don’t take naps and don’t sleep well… I feel relatively calm and just completed a second session for 14 minutes. I am now pretty tired.
I don’t know the outcome of this process, but I have a strong feeling that neurofeedback is going to help rid me of my low self esteem, my rough edges and though I am really tired, I think this is going to really make some good changes. It already did something, as normally looking at a computer screen would never make me take a nap.
More Good Results
On April 8, I had more good results: I did a few more BrainPaint® sessions throughout the day. Then last night I slept the best I have in months!
On April 20, I did an “Alpha-Theta” session on BrainPaint® and had a rather weird experience so here’s what happened:
I am stuck inside an ostrich shell. I am really stuck. I am little but grown. I am pushing on the shell. It doesn’t move and all around me is space …. lots of space.. me in a shell… then I flash into the basement…. it is dark but there is a window a small window that is in the basement and I look outside trying to see the outside where it is light and bright and trees and leaves and I am stuck…
I don’t fight, I just flash back into the eggshell… then I think I cannot push this open… I will try to melt it away into infinity ..the infinity of equanimity ….. then it was done….
I suppose this is what we experience in the early sessions.
Coming July 24: Part 2 of Tina’s amazing report
———————————
Kathy’s blogs and Guest Blogs explore the journey of recovery from childhood trauma by learning about Adult Attachment Disorder in teens and adults, Adult Attachment Theory, and the Adverse Childhood Experiences (ACE) Study.
Can School Heal Children in Pain? – Guest Blog by “Paper Tigers” Director James Redford, original date June 3 (photo courtesy of Mr. Redford).
After learning about the overwhelming effects of childhood trauma, I decided to make a film about a school that’s adopted a “trauma-informed” lens.
Documentaries are no walk in the park. They take a lot of time and money; they have a way of making a mockery out of your narrative plans…
Why bother? It’s a good question. For me, I have one simple bar that all my films must clear: an “oh my God!” moment. If a story does not elicit that reaction from deep within my bones, I don’t do it. I count on that sense of awe, concern, wonder, and alarm to carry me through the long haul of making the film…
After three years of hard work and uphill battles, my latest documentary film, Paper Tigers, premiered last week [May 28] at the Seattle International Film Festival. And yet it seems like yesterday that I first encountered the explosive research that linked poor health to childhood trauma.
I didn’t know that adverse childhood experiences — like assault, emotional abuse, observing domestic violence — could fundamentally alter a child’s body and brain. These kids are at risk for every single major disease, including (but not limited to) cancer, diabetes, high blood pressure, and cardiovascular disease. That risk doesn’t include the increased likelihood of “self-soothing behaviors” like smoking, drinking, eating too much food, doing too many drugs, having too much sex.
Put that all together and you have the underpinnings for some of the greatest societal challenges we face. It quickly became clear that social support systems require a deeper understanding of adverse childhood experiences….
The good news is that there are schools, clinics, courts, and communities that are starting to adopt a “trauma-informed” lens.
Kathy’s blogs and Guest Blogs explore the journey of recovery from childhood trauma by learning about Adult Attachment Disorder in teens and adults, Adult Attachment Theory, and the Adverse Childhood Experiences (ACE) Study.
The Adverse Childhood Experiences (ACE) Study showed that for 17,337 patients, childhood trauma correlated to serious adult medical conditions. “Contrary to conventional belief," says co-Director Vincent Felitti, MD, "time does not heal all wounds, since humans convert traumatic emotional experiences in childhood into organic disease later in life.”
FEATURED BOOKS – QUOTES
"Too many Americans are spurred to achieve, rather than to attach." --A General Theory of Love
"Trying to fix the heart using the head, is like trying to paint with a hammer - it only makes a mess."
"You can be strong - or you can be human."
-- Grief Recovery Handbook
"Gosh, I shoulda checked the milligramage! Oh, well, Live and Learn." -- Working Girl
"Any book you haven't thrown across the room at least once because it smashed your world view, probably isn't worth a long shelf life." -- Kathy
"Mental health. For everything else there's MasterCard." -- Kathy
 CLICK to BUY “Don’t Try This Alone”
CLICK to BUY “Don’t Try This Alone”